You know how every piece of a broken hologram becomes a smaller hologram and projects the whole thing? There.
I could waste more of your time with blah, but let’s be honest here.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
I can’t find the irony because I’m distracted by the facts. The highlights in the text are mine, they are the key.
Flipping a Switch Inside the Head
With new technology, scientists are able to exert wireless control over brain cells of mice with just the push of a button. The first thing they did was make the mice hungry.
By W. Wayt Gibbs, APRIL 1, 2017
READY YOUR TINFOIL HATS—mind control is not as far-fetched an idea as it may seem. In Jeffrey M. Friedman’s laboratory, it happens all the time, though the subjects are mice, not people.
Friedman and his colleagues have demonstrated a radio-operated remote control for the appetite and glucose metabolism of mice—a sophisticated technique to wirelessly alter neurons in the animals’ brains. At the flick of a switch, they are able to make mice hungry—or suppress their appetite—while the mice go about their lives normally. It’s a tool they are using to unravel the neurological basis of eating, and it is likely to have applications for studies of other hard-wired behaviors.
Friedman, Marilyn M. Simpson Professor, has been working on the technique for several years with Sarah Stanley, a former postdoc in his lab who now is assistant professor at the Icahn School of Medicine at Mount Sinai, and collaborators at Rensselaer Polytechnic Institute. Aware of the limitations of existing methods for triggering brain cells in living animals, the group set out to invent a new way. An ideal approach, they reasoned, would be as noninvasive and non-damaging as possible. And it should work quickly and repeatedly.
Although there are other ways to deliver signals to neurons, each has its limitations. In deep-brain stimulation, for example, scientists thread a wire through the brain to place an electrode next to the target cells. But the implant can damage nearby cells and tissues in ways that interfere with normal behavior. Optogenetics, which works similarly but uses fiber optics and a pulse of light rather than electricity, has the same issue. A third strategy—using drugs to activate genetically modified cells bred into mice—is less invasive, but drugs are slow to take effect and wear off.
The solution that Friedman’s group hit upon, referred to as radiogenetics or magnetogenetics, avoids these problems. With their method, published last year in Nature, biologists can turn neurons on or off in a live animal at will—quickly, repeatedly, and without implants—by engineering the cells to make them receptive to radio waves or a magnetic field.
“In effect, we created a perceptual illusion that the animal had a drop in blood sugar.”
“We’ve combined molecules already used in cells for other purposes in a manner that allows an invisible force to take control of an instinct as primal as hunger,” Friedman says.
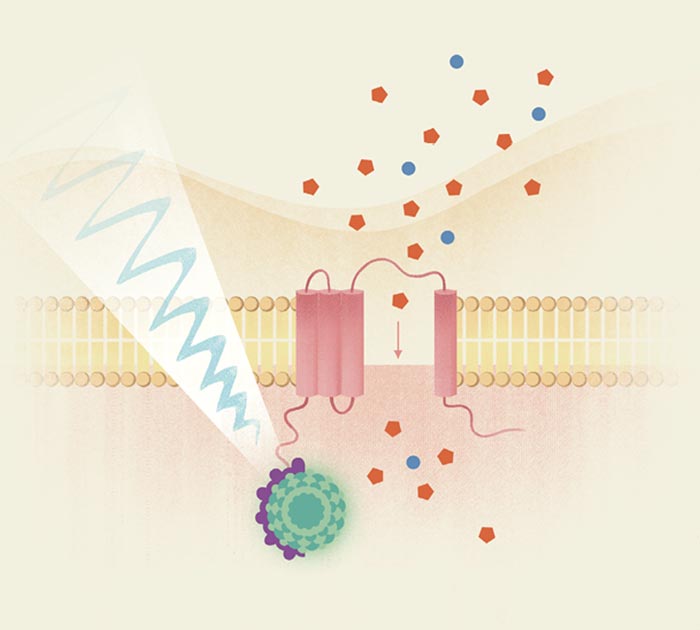
The method links five very different biological tools, which can look whimsically convoluted, like a Rube Goldberg contraption on a molecular scale. It relies on a green fluorescent protein borrowed from jellyfish, a peculiar antibody derived from camels, squishy bags of iron particles, and the cellular equivalent of a door made from a membrane-piercing protein—all delivered and installed by a genetically engineered virus. The remote control for this contraption is a modified welding tool (though a store-bought magnet also works).
The researchers’ first challenge was to find something in a neuron that could serve as an antenna to detect the incoming radio signal or magnetic field. The logical choice was ferritin, a protein that stores iron in cells in balloon-like particles just a dozen nanometers wide. Iron is essential to cells but can also be toxic, so it is sequestered in ferritin particles until it is needed. Each ferritin particle carries within it thousands of grains of iron that wiggle around in response to a radio signal, and shift and align when immersed in a magnetic field. We all have these particles shimmying around inside our brain cells, but the motions normally have no effect on neurons.
Friedman and Stanley, with equipment they use to send radio waves. Photo by Zachary Veilleux
Friedman’s team realized that they could use a genetically engineered virus to create doorways into a neuron’s outer membrane. If they could then somehow attach each door to a ferritin particle, they reasoned, they might be able to wiggle the ferritin enough to jostle the door open. “The ‘door’ we chose is called TRPV1,” says Stanley. “Once TRPV1 is activated, calcium and sodium ions would next flow into the cell and trigger the neuron to fire.” The bits borrowed from camels and jellyfish provided what the scientists needed to connect the door to the ferritin (see How to outfit a brain sidebar, right).
Once the team had the new control mechanism working, they put it to the test. For Friedman and Stanley, whose goal is to unravel the biological causes of overeating and obesity, the first application was obvious: Try to identify specific neurons involved in appetite. The group modified glucose-sensing neurons—cells that are believed to monitor blood sugar levels in the brain and keep them within normal range—to put them under wireless control. To accomplish this, they inserted the TRPV1 and ferritin genes into a virus and—using yet another genetic trick—injected them into the glucose-sensing neurons. They could then fiddle with the cells to see whether they are involved, as suspected, in coordinating feeding and the release of hormones, such as insulin and glucagon, that keep blood glucose levels in check.
HOW TO OUTFIT A BRAIN FOR RADIO CONTROL Scientists have come up with a clever way to control neurons via radio by cobbling together genes from humans, camels, and jellyfish. They use an engineered virus to install a door into each target neuron’s outer membrane, then jostle the door open using ferritin particles that respond to strong radio signals. Once the door opens, calcium ions pour into the cell and trigger the neuron to fire. 1. To install the radiogenetics system into neurons, the scientists equipped an adenovirus with the various genes needed to make the system work. Then they squirted the modified virus onto the brain cells they wanted to alter. 2. One of the added genes produces TRPV1, a protein that normally helps cells detect heat and motion. Within each neuron, the TRPV1 protein (pink) embeds itself into the cell’s outer membrane. Like a door, it can change shape to open or shut an ion channel. To add a knob to the door, the researchers stitched TRPV1 to a “nanobody” (violet)—an unusually simple variety of antibody found in camels. 3. Iron-filled ferritin particles (green) serve as the system’s sensor. To allow them to grab onto the nanobody doorknob, the researchers tacked on a gene for GFP—a jellyfish protein that glows green under ultraviolet light. By design, the nanobody and GFP stick together tightly. The system is now connected. When exposed to strong radio waves or magnetic fields, the ferritin particles wiggle, the ion channel opens, and calcium ions (red) flow in to activate the cell.
Once the virus had enough time to infect and transform the target neurons, the researchers switched on a radio transmitter tuned to 465 kHz, a little below the band used for AM radio.
The neurons responded. They began to fire, signaling a shortage of glucose even though the animal’s blood sugar levels were normal. And other parts of the body responded just as they would to a real drop in blood sugar: insulin levels fell, the liver started pumping out more glucose, and the animals started eating more. “In effect,” Friedman says, “we created a perceptual illusion that the animal had low blood glucose even though the levels were normal.”
Inspired by these results, the researchers wondered if magnetism, like radio waves, might trigger ferritin to open the cellular doors. It did: When the team put the mice cages close to an MRI machine, or waved a rare-earth magnet over the animals, their glucose-sensing neurons were triggered.
Stimulating appetite is one thing. Could they also suppress it? The group tweaked the TRPV1 gene so it would pass chloride, which acts to inhibit neurons. Now when they inserted the modified TRPV1 into the neurons, the rush of chloride made the neurons behave as if the blood was overloaded with glucose. Insulin production surged in the animals, and they ate less. “This seems to indicate clearly that the brain as well as the pancreas is involved in glucose regulation,” Friedman says.
Friedman and Stanley hope that biologists will be able to use the remote-control system to tackle a range of neural processes other than appetite. And beyond being a basic research tool, the method could potentially lead to novel therapies for brain disorders.
For example, one could imagine using it to treat Parkinson’s disease or essential tremor—conditions that are sometimes treated by deep brain stimulation, via wires implanted into patients’ brains and connected to a battery pack tucked into the chest. Potentially, it would be less invasive to inject the crippled virus into the same spot of the brain and let it permanently modify the cells there, making them responsive to wireless control.
In theory, it might also be possible to make a patient’s own cells receptive to electromagnetic waves by removing them from the body, delivering TRPV1 and ferritin, and then putting the cells back, Friedman says. This would be a protocol not unlike those currently used in stem cell treatments and some cancer immunotherapies, in which patients’ own cells are engineered and reimplanted back into their bodies.
At this point, however, the system’s clinical usefulness is a question of speculation. “We are a long way from using it in humans for medical treatments,” Friedman says. “Much would need to be done before it could even be tested.”
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Can’t wait to make a video and see if YouTube bans this!
Remember “The Good Cabal” who “fortified the 2020 elections” in US, according to TIME? You think they stopped after successfully hi-jacking the US Government? However, this group below has been described by mainstream media as “The Good Club”. Right.
Stacy Palmer, editor of the Chronicle of Philanthropy, said the summit was unprecedented. “We only learnt about it afterwards, by accident. Normally these people are happy to talk good causes, but this is different – maybe because they don’t want to be seen as a global cabal,” he said.
May 26, 2009, 11:57 AM ET
Billionaires Try to Shrink World’s Population, Report Says
Last week’s meeting of the Great and the Good (or the Richest and Richer) was bound to draw criticism.
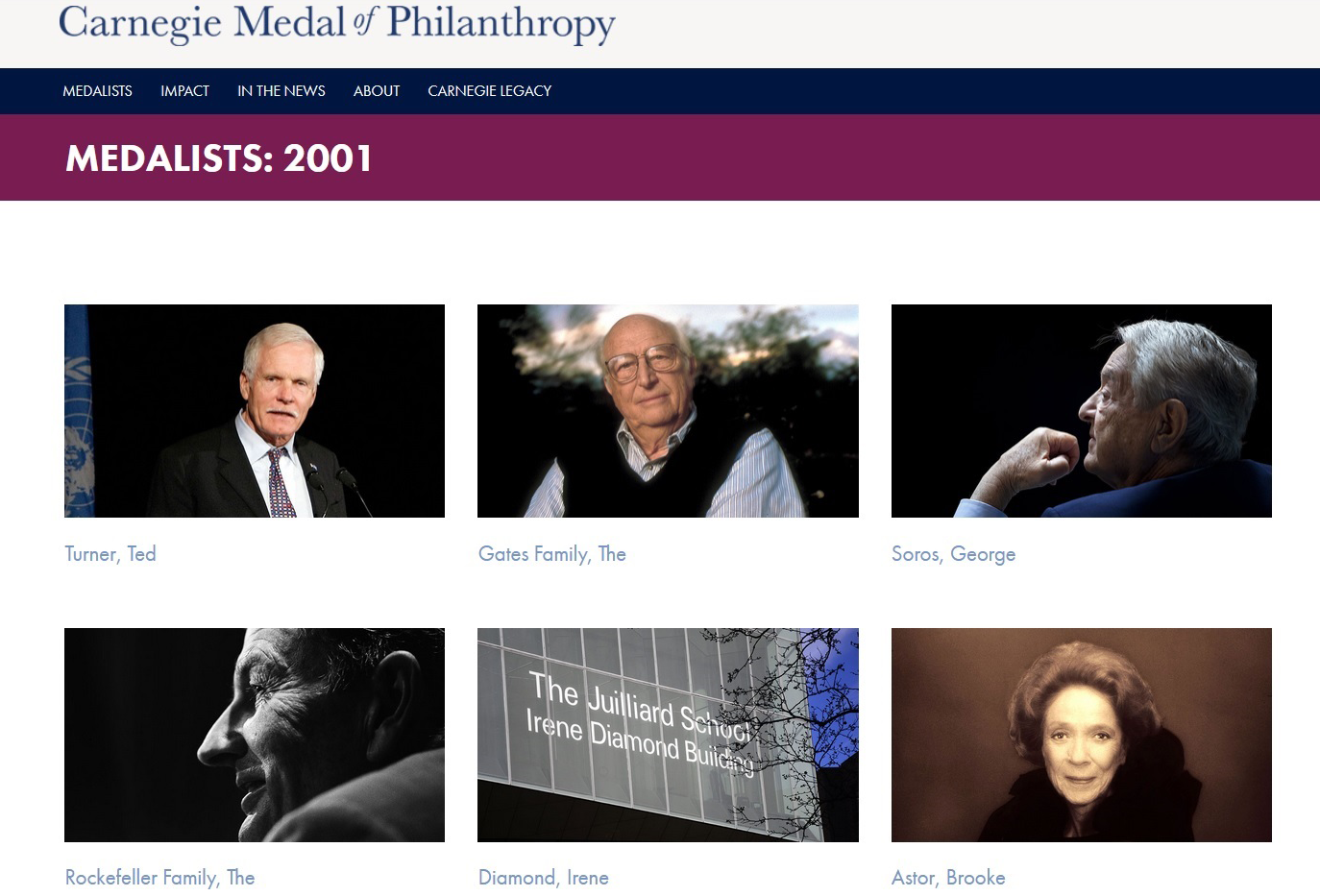
The New York meeting of billionaires Bill Gates, Warren Buffett, David Rockefeller, Eli Broad, George Soros, Ted Turner, Oprah, Michael Bloomberg and others was described by the Chronicle of Philanthropy as an informal gathering aimed at encouraging philanthropy. Just a few billionaires getting together for drinks and dinner and a friendly chat about how to promote charitable giving.
There was no agenda, we were told. And no plan for a follow-up meeting.
But in an age of fallen wealth idols, it was inevitable that a meeting of billionaire minds would draw scrutiny. Surely all that money and power in one room had to spell trouble for the rest of us.
An article in the Times of London, headlined “Billionaire Club in Bid to Curb World Population,” said the issues discussed in the top-secret meeting included health care, education and–by far the most controversial–slowing the global population growth.
“Taking their cue from Gates they agreed that overpopulation was a priority,” the article said, adding that “this could result in a challenge to some Third World politicians who believe contraception and female education weaken traditional values.”
Such a stand wouldn’t be surprising. Mssrs. Gates, Buffett and Turner have been quietly worrying about Malthusian population problems for years. Mr. Gates in February outlined a plan to try to cap the world’s population at 8.3 billion people, rather than the projected 9.3 billion at which the population is expected to peak.
But some right-leaning blogs have started attacking the billionaires as forming a kind of secret sterilization society or giant ATM to fund abortions. It fed into time-honored fears of the rich using their wealth to reshape mankind in its preferred image. Some are raising the specter of eugenics.
I am not taking a stand on population control. But from what I was personally told about the meeting–and what the Times spells out further down in its story–population control was just one of many items raised during the meeting, as each philanthropist talked about what they were working on. It wasn’t the reason for meeting and there are no real plans for a follow-up confab.
The notion that this secret gathering was aimed mostly at shrinking the world’s population just doesn’t ring true.
That said, almost all of the attendees are politically liberal. Do you think this Star Chamber of Philanthropists is something to worry about or something to be grateful for?
Oprah Winfrey’s charity challenge
Eleven of the world’s wealthiest people, including Warren Buffett and Bill Gates, met in secret a fortnight ago to discuss the future of philanthropy in light of the continued global economic crisis.
By The Telegraph UK Last Updated: 7:41PM BST 21 May 2009
Other attendees included Oprah Winfrey, the billionaire chat show host, Michael Bloomberg, mayor of New York, Ted Turner, the media mogul, and George Soros, the man who “broke the Bank of England” in 1992.
Although details of the meeting are only now emerging, it is believed the group met to brainstorm how best to bolster charitable giving in spite of the recent reduction in wealth.
Despite market conditions, the 11 attendees still share a combined fortune of $120bn (£76bn), based on the Forbes 2009 list of the world’s richest people.
The meeting was held on May 5, at the private residence of the president of Rockefeller University on New York’s exclusive Upper East Side.
It is not known if the attendees discussed working together on a charitable basis, although all present have been involved in philanthropy in some shape or form.
Mr Gates has bestowed the majority of his $37bn fortune to the Bill & Melinda Gates Foundation, while Mr Soros last week pledged $50m to the Robin Hood Foundation.
Article deleted and retrieved with the Wayback Machine:
Wednesday May 20, 2009 America’s Top Philanthropists Hold Private Meeting to Discuss Global Problems By Chronicle of Philanthropy
In a quiet meeting closed to the news media and the public, Bill Gates, David Rockefeller Sr., Oprah Winfrey, and other leading philanthropists met in New York this month to discuss ways to promote charitable giving and make their philanthropy more effective in fighting problems at home and abroad. The unusual event, which occurred May 5 at Rockefeller University in New York, was an unprecedented gathering of the world’s wealthiest — and most generous — people. Together, the philanthropists in the room have committed a total of more than $72.5-billion to charitable causes since 1996, according to Chronicle of Philanthropy tallies. While the meeting and its hush-hush nature has triggered intense speculation by the news media about what was discussed, Patricia Q. Stonesifer, former chief executive of the Bill & Melinda Gates Foundation, said it was simply a gathering of people who have a common passion for helping others. “A group of philanthropists came together to discuss their giving,” said Ms. Stonesifer, who attended the meeting. “There’s really no secret about that. It was an informal get-together and a chance to exchange ideas about what motivates them and what they have learned so far.” “There was an enormous amount of enthusiasm and excitement around their giving and that was a very big part of what they were there for,” she added. Among the high-profile participants were Ted Turner, Warren E. Buffett, George Soros, Peter G. Peterson, Eli Broad, and New York City Mayor Michael R. Bloomberg. (All of those philanthropists have appeared at one time on The Chronicle’s ranking of America’s most-generous donors.)Mr. Buffett, Mr. Rockefeller, and Mr. Gates called together the elite group, sending a short letter of invitation to each of the guests. Mr. Rockefeller arranged the location — the private Manhattan residence of Rockefeller University’s president. (Mr. Rockefeller is an honorary member of the institution’s Board of Trustees.) Ms. Stonesifer, who helped coordinate the meeting, said it started at 3 p.m. and lasted through dinner. Given the personalities in the room, the meeting touched upon a variety of philanthropy topics, said Ms. Stonesifer, who is currently chairwoman of the Smithsonian Institution’s Board of Regents.“ It was a wide-ranging conversation,” she said, “but they each shared what motivates their giving, their areas of focus of their work, the lessons learned, and thoughts on how we might increase giving.” Indeed, the philanthropic interests represented on that day were rather diverse. For example, Mr. Peterson, co-founder of a private-equity firm, is focused on changing the government’s financing of social programs and other fiscal issues, while Ms. Winfrey has primarily given money to education efforts in South Africa and elsewhere. Ms. Stonesifer — and others who attended the event — declined to say what was specifically talked about. The former Gates foundation leader did say that the attendees are not working on a major collaborative charitable project but do plan to continue to talk to one another.“ It was a really great discussion, and we agreed to continue the dialogue in the future, but there were no specific action items out of the meeting,” she said. With such a powerful guest list, some blog writers have fixated on the meeting as the origins of some international conspiracy. But Ms. Stonesifer objected to the meeting being described as a “secret” event with mysterious intent.“ It was a private gathering. There are often opportunities for each of these individuals to discuss their giving in public — and they often do. But this really was a conversation among friends and colleagues.” She added: “People are automatically curious about these types of things. But they were all quite matter-of-fact about why they were there. It was like a gathering that you and I have, but it was just a different group of friends and colleagues discussing what they care about.”
But you’re crazy to suspect anything malicious.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
We gave up on our profit shares from masks, if you want to help us, please use the donation button! We think frequent mask use, even short term use can be bad for you, but if you have no way around them, at least send a message of consciousness. Get it here!
Establishment fact-checkers are cognitively retarded and functionally illiterate copy-paste bots who still use Google, this is how you fact-check Stu Peters:
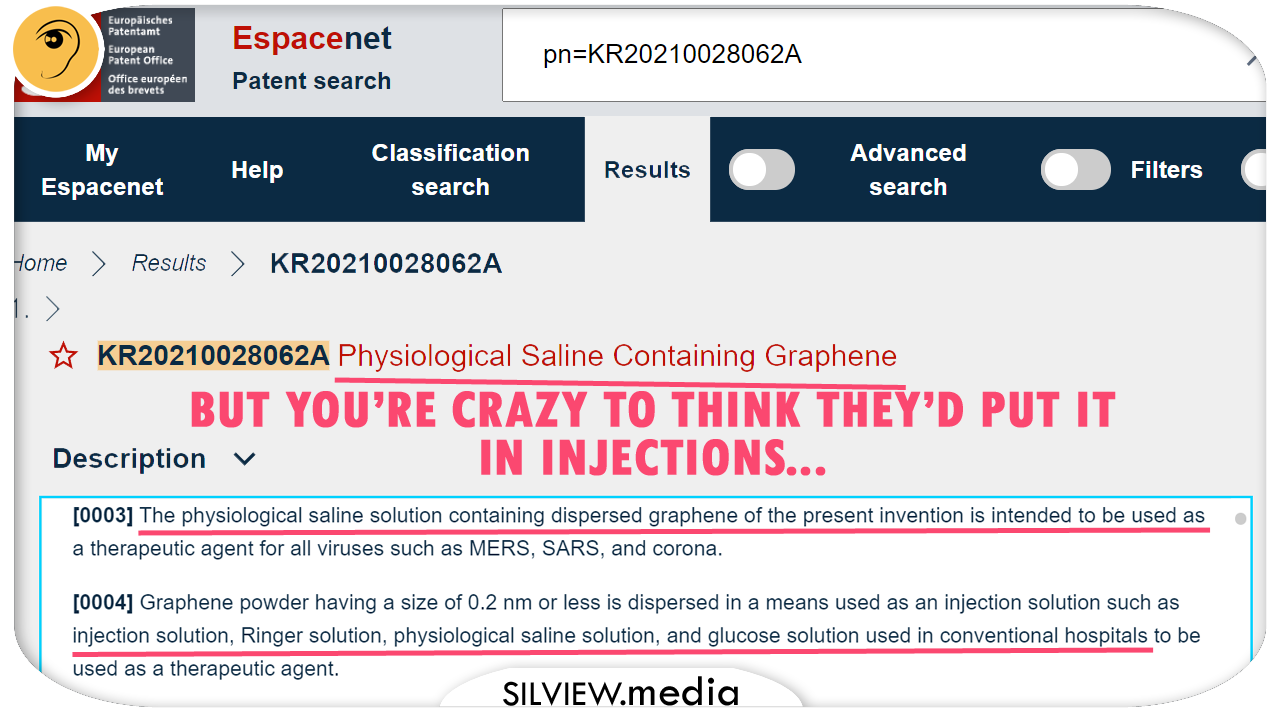
LATER UPDATES: A glimpse into the future or the present?
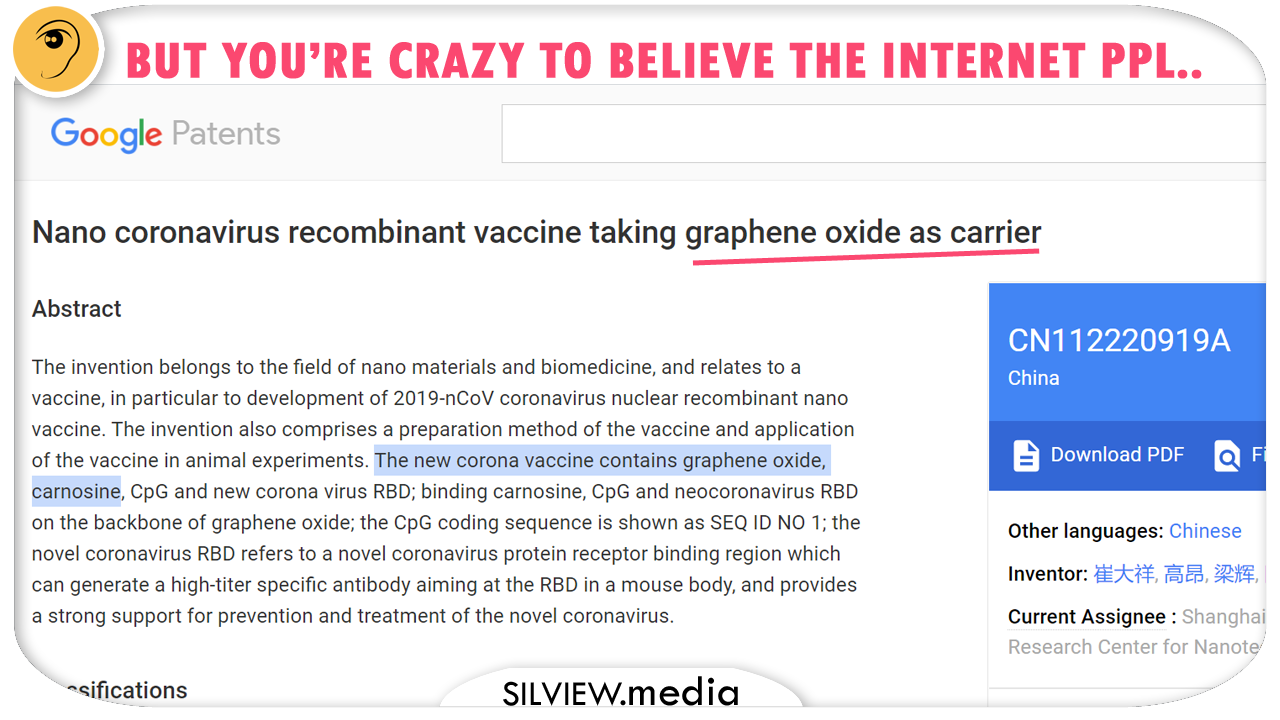
So the people who claim many vaccines are just saline and the people who claim they are just graphene oxide can be right at the same time.
If you are reading this, chances ae you already know of La Quinta Columna researchers and Stu Peters shows that revealed large presence of very toxic graphene in Covid injections. If you don’t, you need to research and catch up with the details, there’s no cheating on the homework anymore.
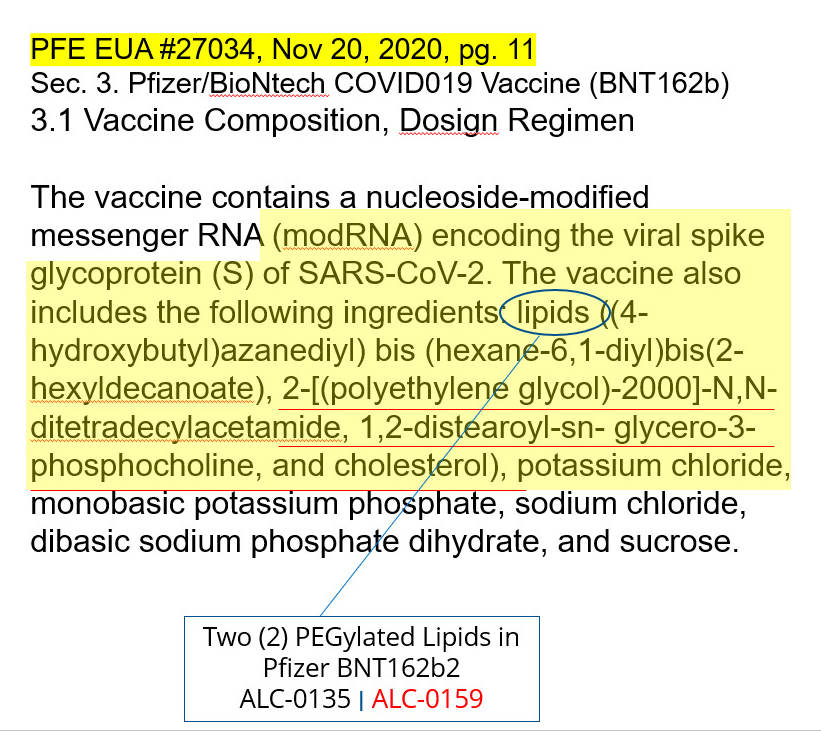
Onw of Stu’s latest deliveries featured a very documented expert and Pharma analyst who formerly worked for Pfizer and revealed the graphene is hiding in the so called PEGs, I’ll explain shortly what these are.
So I went to fact-check this, even though the whistle-blower sounded very compelling and having deep insights in the business.
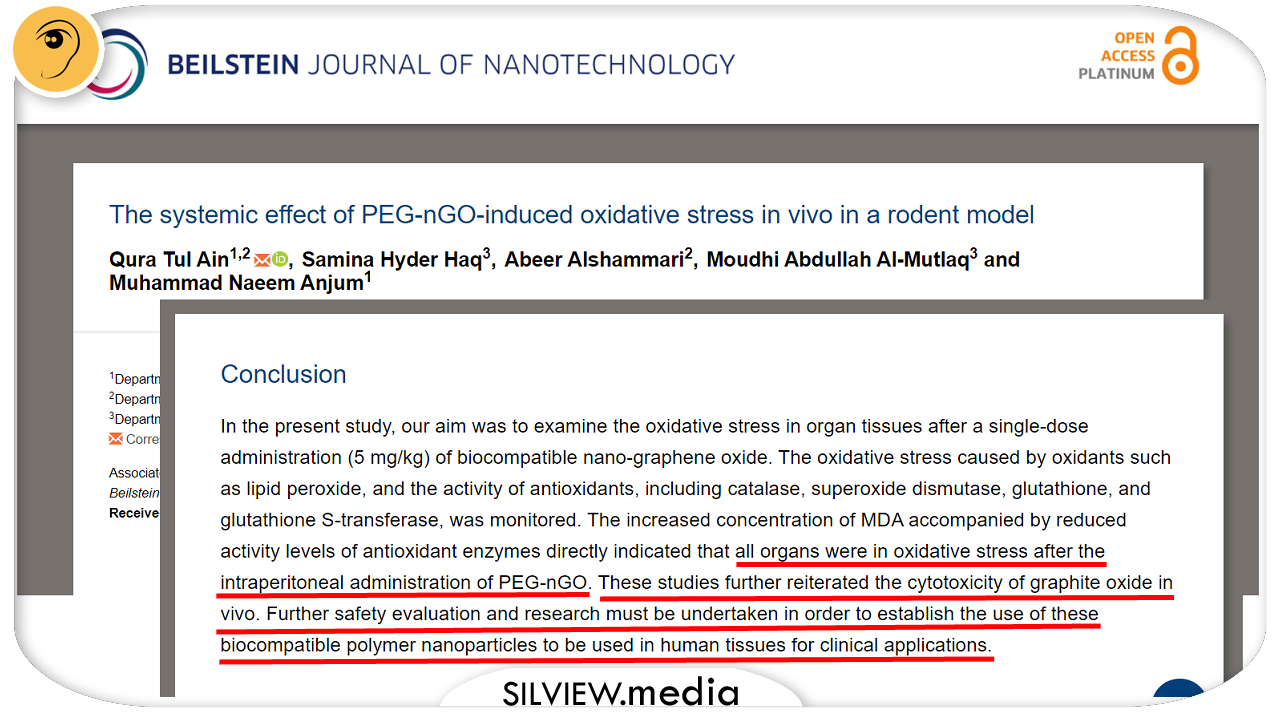
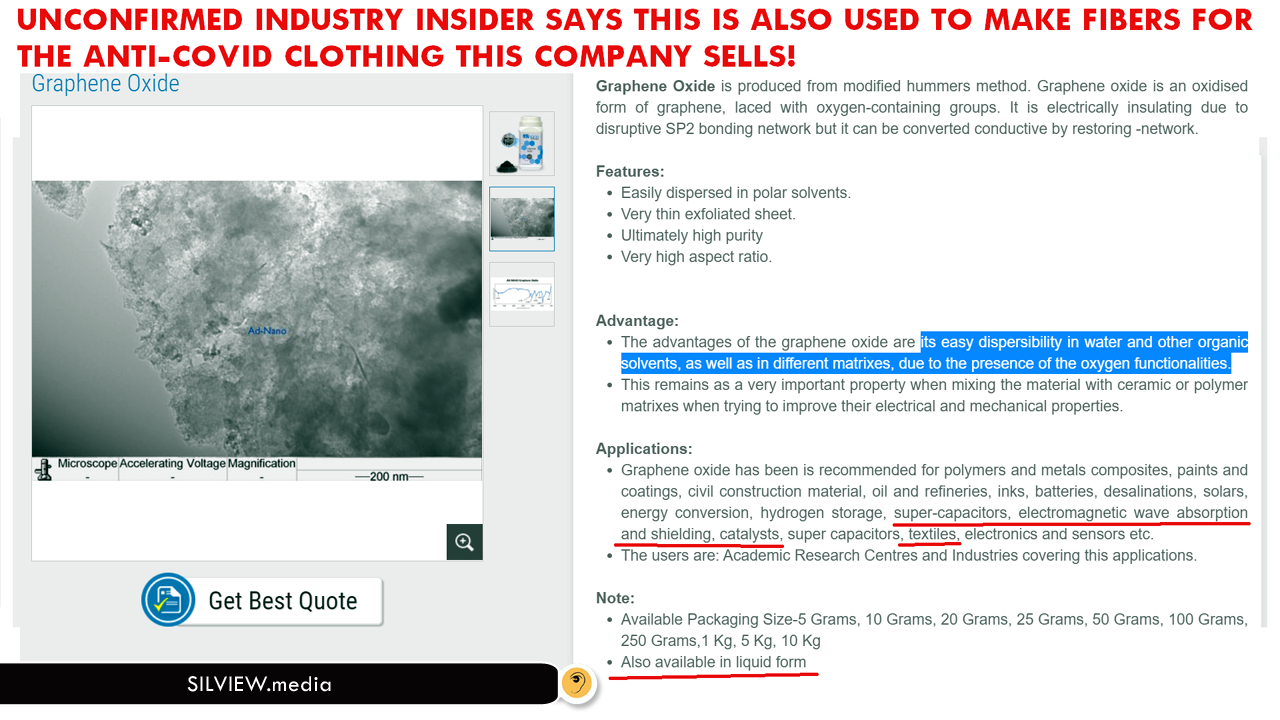
My findings show that they only scratch the surface of a larger problem: As I’ve shown before, graphene has a large spectrum of applications today, most endangering our health. But graphene oxide (GO) is especially toxic and they will pump it in us with other treatments too.
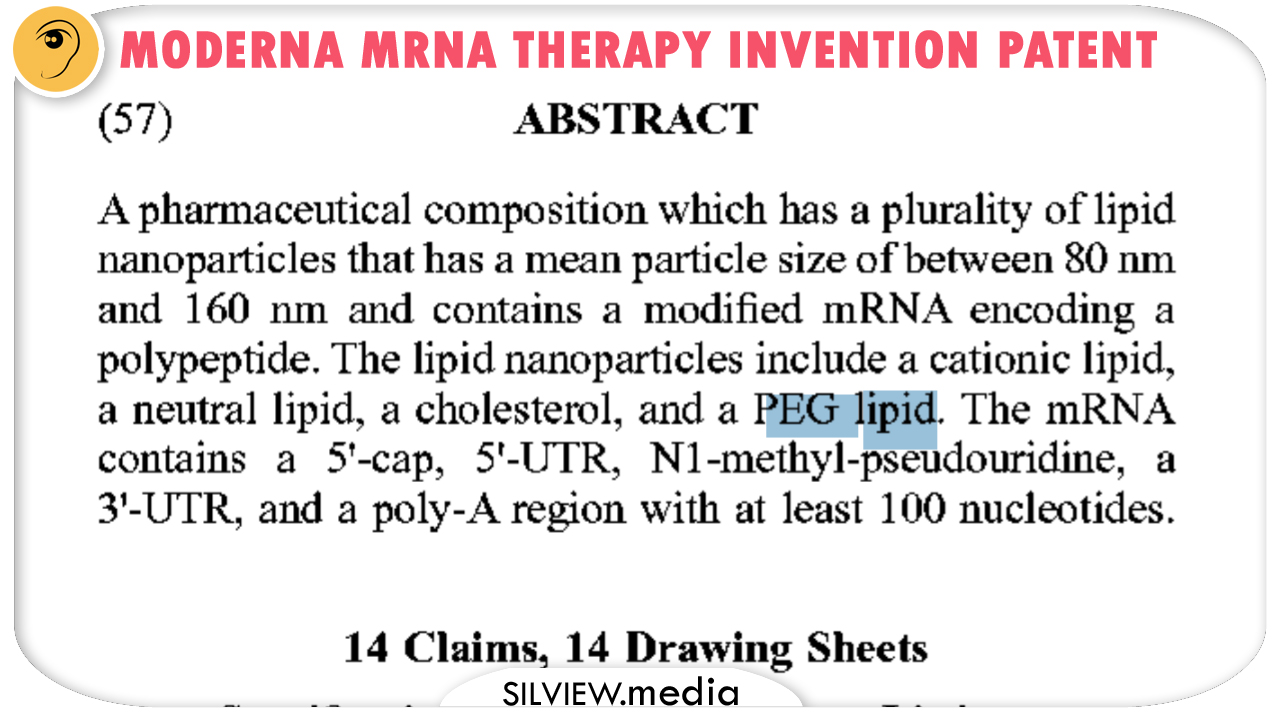
GO-based PEGs have been the new rising star of drug delivery for quite a few years before Covid and they are usually graphene based, as a several studies and invention patents prove beyond doubt. I don’t think there’s any mRNA vaccine that doesn’t use them.
They are not featured in injections inserts as separate ingredient, which they are, but as a process. Yup, they are the PEG in PEGylation. It’s like saying Coca Cola was sweetened instead of listing several sweeteners!
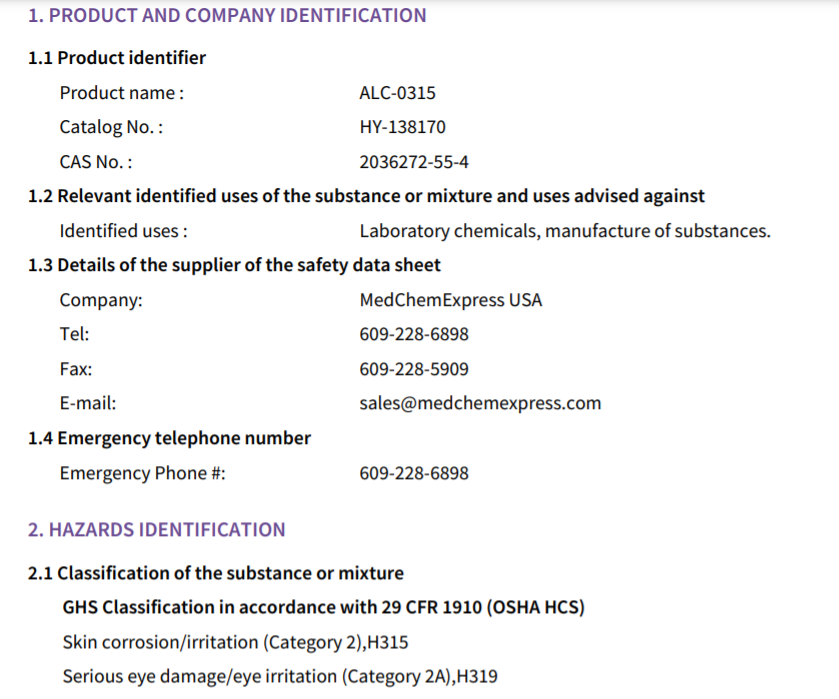
Here you can download the safety Data Sheet for ALC-0135, it’s bad stuff, really corrosive!
Think of an oral drug capsule. The PEG is a high-nanotech version of the capsule fabric, which can do a series of cool tricks, but its mainly roles are to protect the content and help it penetrate tissue/cells and reach specific targets.
Now think the drug insert only lists the content ingredients. not the capsule.
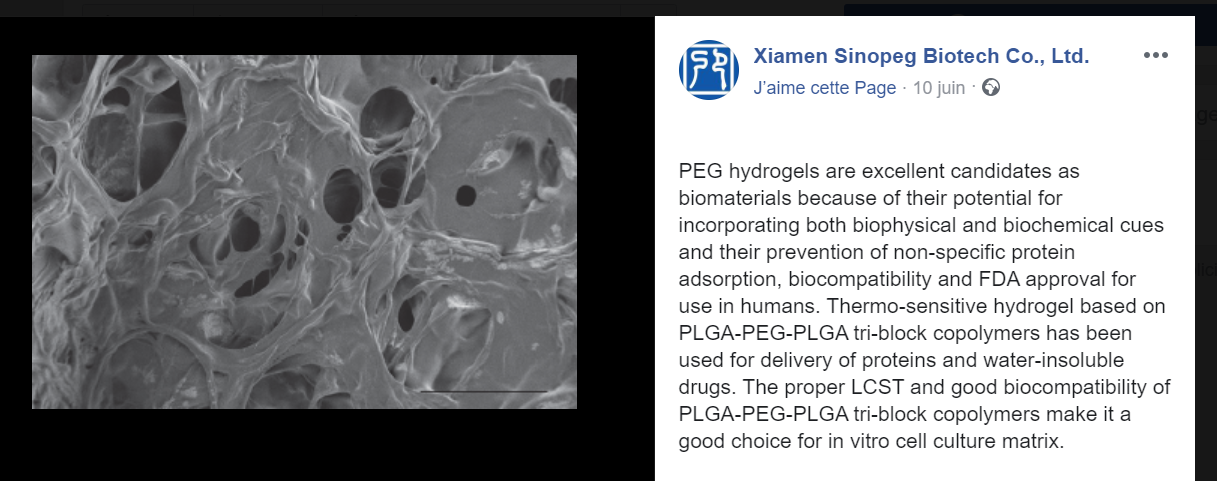
“Poly(ethylene glycol) (PEG), also known as poly(ethylene oxide) (PEO), is an amphiphilic polyether that is soluble both in water and most organic solvents. PEG and its derivatives are among the few polymers approved for medical uses by the FDA.
Functionalized PEG, also named activated PEG, is a family of PEG derivatives decorated with functional groups. Funtionalized PEGs are used broadly for drug PEGylation, polymer engineering, nantechnology, biotechnology, and biomedical engineering.” This is the description given by Sinopeg, Chinese company that delivers PEGs for most Covid injection manufacturers.
From their September 2020 blog post we extract more details confirming my earlier claims:
“The coupling of PEG to protein is also called protein polyglycolization, which is essentially a drug delivery technology. The coupling of activated peg with protein molecules can improve the three-dimensional space state of proteins, resulting in changes in various biochemical properties of proteins. For example, chemical stability increased, half-life prolonged, immunogenicity and toxicity decreased or disappeared, protein solubility increased. SINOPEG is a dynamic science company dedicated to drug delivery systems (DDS). SINOPEG are specialized in the R&D of long acting biopharmaceuticals, developing and manufacturing of block copolymers, lipids for drug delivery, medical devices, bio-engineering, and other broad uses.
Up to now, the FDA has approved 20 polyglycolic drugs. In addition to monoclonal antibodies, polyglycolic drugs have become the most powerful drug development technology. As a leading company in polyethylene glycol derivatives (PEGs), SINOPEG is capable of supplying small to large quantities of rich selection of PEG derivative products with unique molecular designs (chemical structure, molecular weights (MW)) and exceptional product quality control to serve bio-technology and pharmaceutical companies and research organizations worldwide.”
At this point, you’re probably asking when is graphene coming in. I got you covered:
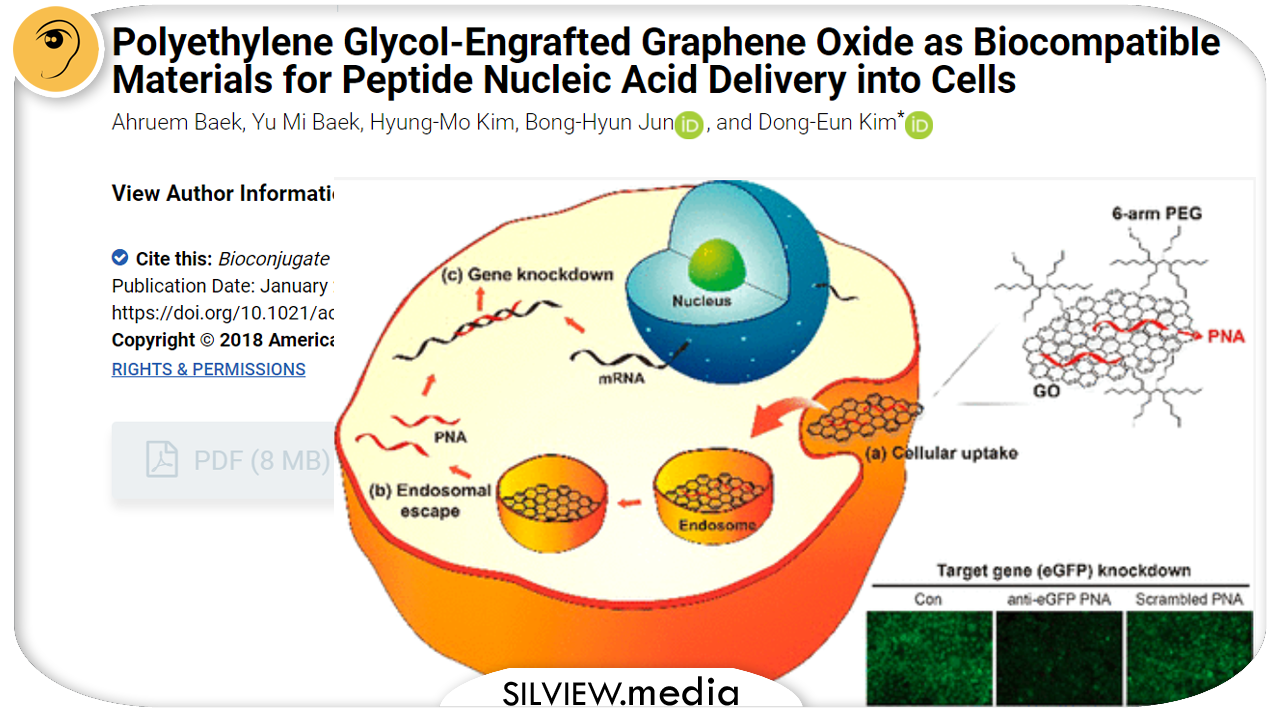
Graphene oxide (GO) is known to strongly bind single-stranded nucleic acids with fluorescence quenching near the GO surface. However, GO exhibits weak biocompatibility characteristics, such as low dispersibility in cell culture media and significant cytotoxicity. To improve dispersibility in cell culture media and cell viability of GO, we prepared nanosized GO (nGO) constructs and modified the nGO surface using polyethylene glycol (PEG-nGO). Single-stranded peptide nucleic acid (PNA) was adsorbed onto the PEG-nGO and was readily desorbed by adding complementary RNA or under low pH conditions. PNA adsorbed on the PEG-nGO was efficiently delivered into lung cancer cells via endocytosis without affecting cell viability. Furthermore, antisense PNA delivered using PEG-nGO effectively downregulated the expression of the target gene in cancer cells. Our results suggest that PEG-nGO is a biocompatible carrier useful for PNA delivery into cells and serves as a promising gene delivery tool.
HEY, KIDS, WANNA BUY SOME LETHAL INJECTIONS AMMO? HERE’S YOUR LINK!
Polymerase chain reaction (PCR), a versatile DNA amplification method, is a fundamental technology in modern life sciences and molecular diagnostics. After multiple rounds of PCR, however, nonspecific DNA fragments are often produced and the amplification efficiency and fidelity decrease. Here, we demonstrated that poly(ethylene glycol)-engrafted nanosized graphene oxide (PEG-nGO) can significantly improve the PCR specificity and efficiency. PEG-nGO allows the specificity to be maintained even after multiple rounds of PCR, allowing reliable amplification at low annealing temperatures. PEG-nGO decreases the nonspecific annealing of single-stranded DNA (ssDNA), such as primer dimerization and false priming, by adsorbing excess primers. Moreover, PEG-nGO interrupts the reannealing of denatured template DNA by preferentially binding to ssDNA. Thus, PEG-nGO enhances the PCR specificity by preferentially binding to ssDNA without inhibiting DNA polymerase, which is analogous to the role of ssDNA binding proteins.
A method and process to make and use cotton-tipped electrochemical immunosensor for the detection of corona viruses is described. The immunosensor were fabricated by immobilizing the virus antigens on carbon nanofiber-modified screen printed electrodes which were functionalized by diazonium electrografting and activated by EDC/NHS chemistry. The detection of virus antigens were achieved via swabbing followed by competitive assay using fixed amount of antibody in the solution. Ferro/ferricyanide redox probe was used for the detection using square wave voltammetric technique. The limits of detection for our electrochemical biosensors were 0.8 and 0.09 pg/ml for SARS-CoV-2 and MERS-CoV, respectively indicating very good sensitivity for the sensors. Both biosensors did not show significant cross reactivity with other virus antigens such as influenza A and HCoV, indicating the high selectivity of the method.
BACKGROUND
The newly identified severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the last discovered member of the corona viruses that cause serious human respiratory infections. Other types of corona viruses were previously known such as the Middle East respiratory syndrome coronavirus (MERS-CoV), SARS-CoV1, HCoV-OC43, HCoV-229E, HCoV HKU1 and HCoV NL63. Since its first identification in China in 2019 until present, SARS-CoV-2 has spread globally causing significant morbidity and mortality. COVID-19; the disease caused by SARS-CoV-2; was declared as pandemic by the world health organization on March 2020. Until now, there are no available vaccines or drugs proven to treat COVID 19. Therefore, the timely detection of SARS-CoV-2, is urgently needed to effectively control the rapid spread of the infection.
The testing of the virus can be achieved by reverse transcription polymerase chain reaction (RT-PCR) test, detection of antigens, or by serological testing (the detection of the virus antibody). However, the serological tests are not reliable for the early diagnosis of SARS-CoV-2 infection due to the relatively long delay between infection and seroconversion. Molecular diagnosis using RT-PCR is the primary used method for the detection of corona viruses. However, PCR takes relatively long time for analysis (minimum of 3 hours), and requires several steps including the collection of the specimens by swabbing, the transport of the sample into a solution and extraction of the viral RNA before amplification. Moreover, RT-PCR is relatively expensive which hindered its wide applicability for population scale diagnosis of SARS-CoV-2, particularly in low and middle income countries. Thus, sensitive, rapid and accurate diagnostic methods based on the direct detection of the viral antigens without pretreatment is highly demanded to control the COVID 19 outbreak. There are four main structural antigens for corona viruses: nucleocapsid (N), spike (S), matrix (M), and envelope (E). Among them, the S and N proteins have the potential to be used as biomarkers because they can distinguish different types of corona viruses.
Several diagnostic methods are being developed for the detection of COVID 19. Biosensors have been widely used for many diagnostic applications showing fast, easy and reliable detection. Until now, only few biosensors have been developed for SARS-CoV-2 such as the graphene-based field-effect transistor (FET) biosensor reported by Seo. et al. The FET immunosensor was used for the detection of SARS-CoV-2 using spike 51 protein as biomarker. Plasmonic photothermal biosensors for SARS-CoV-2 through nucleic acid hybridization have been also developed. Half-strip lateral flow assays (LFA) for the detection of N protein was reported. However, LFA provide qualitative or semi-quantitative results and more work is still required to develop more accurate detection methods.
Electrochemical biosensors are one of the most popular types of biosensors which offer several advantages such as the low cost, capability of miniaturization, high sensitivity and selectivity. These advantages make them ideal for use as point-of-care devices for diagnostic applications. Electrochemical biosensors have been widely integrated with carbon nanostructures to fabricate highly sensitive devices. Carbon nanofiber (CNF) is one of the materials that showed excellent applications in biosensors because of its large surface area, stability and ease of functionalization.
Cotton swabs have been recently used in the fabrication of immunoassays for the detection of different pathogens. In these assays, the colorimetric detection was achieved based on visual discrimination of the color change. These assays are simple, fast and easy to perform. However, they only give qualitative or semi-quantitative results. Thus, more accurate methods are still required.
Want some graphene nano-flakes with your milk?
COMPOSITION FOR PCR CONTAINING A POLYETHYLENE GLYCOL-ENGRAFTED NANO-SIZED GRAPHENE OXIDE United States Patent Application 20180155765
BACKGROUND
1. Field of the Invention
The present invention relates to a composition for PCR including polyethylene glycol-engrafted nano-sized graphene oxide (PEG-nGO), the composition for PCR being capable of increasing the efficiency and specificity of PCR and shortening PCR time, and a PCR method using the same.
2. Discussion of Related Art
Polymerase chain reaction (PCR) is a method of artificially amplifying DNA and is an indispensable technology in modern biotechnology and molecular biology. PCR is widely used in diagnostics, gene manipulation, biosensors, and a variety of fields. However, the specificity and efficiency of PCR may be reduced due to unintended (re)annealing of single stranded DNA (e.g., primer dimerization, incorrect primer binding, and reannealing of PCR amplicons). Nonspecific primer binding in PCR steps may result in generation of a large number of nonspecific amplicons, which can be confirmed by agarose gel electrophoresis. That is, smearing of a PCR band, which is observed in an electrophoresed agarose gel, indicates the presence of a large number of DNAs having similar sizes (i.e., nonspecific amplicons). When a DNA template is excessively amplified in PCR and the same primers are used in the second or subsequent PCR, nonspecific amplicons may be generated. To solve these problems, various PCR techniques such as nested PCR have been developed. In the first step of nested PCR, a primer set for amplifying a broad range including a target sequence on a DNA template is used, and in the second step, primer sequences for amplifying only the target sequence are generally used as an inner primer (nested primer) set.
In addition, studies have been conducted to increase the efficiency and specificity of PCR using various nanomaterials such as gold nanoparticles, carbon nanotubes, carbon nanopowder, graphene nanoflakes, cadmium telluride quantum dots, graphene quantum dots, dendrimers, and titanium dioxide. For example, graphene nanoflakes serve to improve PCR efficiency by increasing thermal conductivity of a PCR mixture, and gold nanoparticles are capable of being adsorbed to DNA and proteins to reduce amplification of nonspecific DNA products. However, these methods have a disadvantage that the specificity and efficiency of PCR may not be fundamentally solved when each nanoparticle is present. It is also controversial as to whether gold nanoparticles play a role in increasing the specificity of PCR.
Graphene oxide (GO) refers to a material having a honeycomb-like nanostructure in which carbons are arranged in a hexagonal lattice, and is prepared by oxidizing a single layer of graphite, i.e., graphene. The surface of GO may have various functional groups such as epoxy groups, hydroxyl groups, and carboxyl groups, which allow the GO to be dissolved in a water-soluble solvent. In addition, GO may bind to single-stranded nucleic acids via π stacking interaction and hydrogen bonding, but has low affinity to double-stranded nucleic acids. Based on the functions of GO, GO has been widely applied in various areas such as DNA detection, biosensors based on energy transfer through fluorescence resonance, and real-time monitoring of fluorescently labeled nucleic acids.
However, GO is not soluble in a buffer solution containing Mg2+ and a high salt concentration, such as a PCR buffer, and is adsorbed to proteins such as a DNA polymerase via non-covalent bonding. It is well known that divalent cations such as Mg2+ induce strong crosslinking between GO sheets, allowing the GO sheets to be aggregated. That is, when other salts are added to a PCR sample for buffering, GO sheets may be aggregated by divalent cations such as Mg2+. In addition, it has been reported that GO is bound to proteins to induce protein aggregation, which may distort the structures of proteins and cause the loss of function of proteins. Polyethylene glycol (PEG) is known as a biocompatible polymer that reduces protein adsorption. Recently, to minimize nonspecific protein adsorption and increase the solubility of GO in a solution with a high salt concentration, nano-sized GO (nGO) was prepared, and the surface of the nGO was coated with PEG to prepare PEG-nGO (Non-Patent Document 1). In Non-Patent Document 1, it is disclosed that, when PEG-nGO interacts with a protein, a nano-bio interface may be formed due to PEGylation of the surface of GO, thereby significantly reducing adsorption of the PEG-nGO to the protein. Accordingly, PEG-nGO is attracting attention as a substance capable of interacting with proteins without impairing the structure and function of the proteins.
Therefore, the present inventors have tried to confirm the effect of PEG-nGO on the efficiency and specificity of PCR. During the denaturation step of PCR, polyethylene glycol-engrafted nano-sized graphene oxide (PEG-nGO) was capable of being adsorbed to single-stranded primers and a DNA template. Accordingly, when PEG-nGO was added to a PCR sample and PCR amplification was performed, in an initial PCR process in which an excessive amount of primers was included, primer dimerization was inhibited, and in a late PCR process in which amplified PCR products were accumulated, nonspecific reannealing between the amplified PCR products and other DNA strands was inhibited. Thus, it was confirmed that, when PCR was performed using a composition for PCR including the PEG-nGO of the present invention, the efficiency and specificity of PCR may be improved and PCR time may be shortened as compared with conventional PCR techniques. By confirming these results, the present invention was completed.
Or perhaps you want to find out about GO-based nano-biosensors:
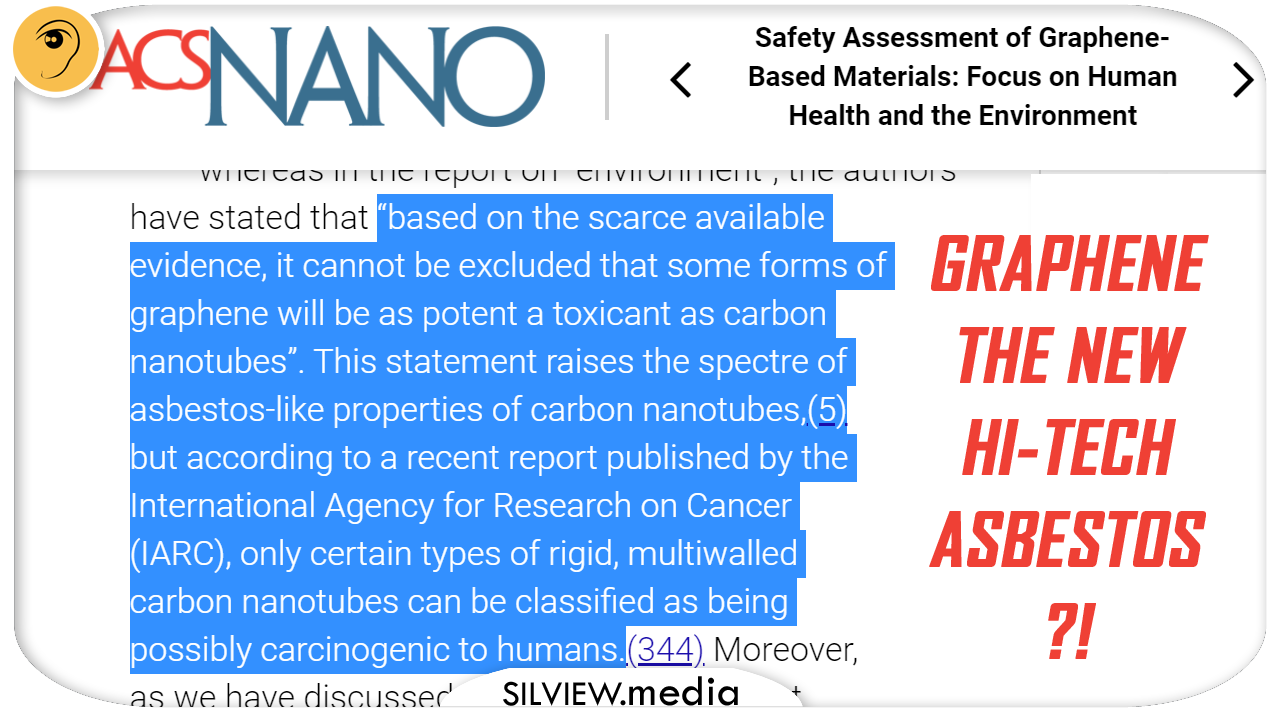
More from the study quoted above: “Furthermore, it is equally important that the material properties are reported in full in papers dealing with (eco)toxicity assessment of GBMs. Can the information that has been collected on safety of GBMs be applied to other 2D materials? We believe that some aspects might be common to all 2D materials, or even to all nanomaterials, while some “postcarbon” 2D materials will likely present with their own specific concerns. For instance, the propensity to dissolve in a biological environment with the release of ionic species that are more biologically/chemically reactive than the parental 2D material is an issue that has not been described for GBMs.(346) Moreover, Guiney et al.(347) recently commented that “with a constantly expanding library of 2D materials, the ability to predict toxicological outcomes is of critical importance” and suggested that high-throughput screening approaches may prove useful in order to elucidate cellular interactions of 2D materials. However, the issue is not so much the low throughput of current approaches as much as the inconsistent design of commonly used toxicity assays and frequent lack of material characterization. Indeed, careful characterization of both the test material and the test system is required, and a proposal was recently put forward for minimum reporting requirements in publications dealing with nanobiointeractions. Though such reporting requirements have not yet been adopted, it is important to discuss these issues in the scientific community. To conclude, the hype that inevitably follows with technological advances should be tempered by sound, science-based assessment of the potential impact on human health and the environment to ensure safe and sustainable development of new products and applications.”
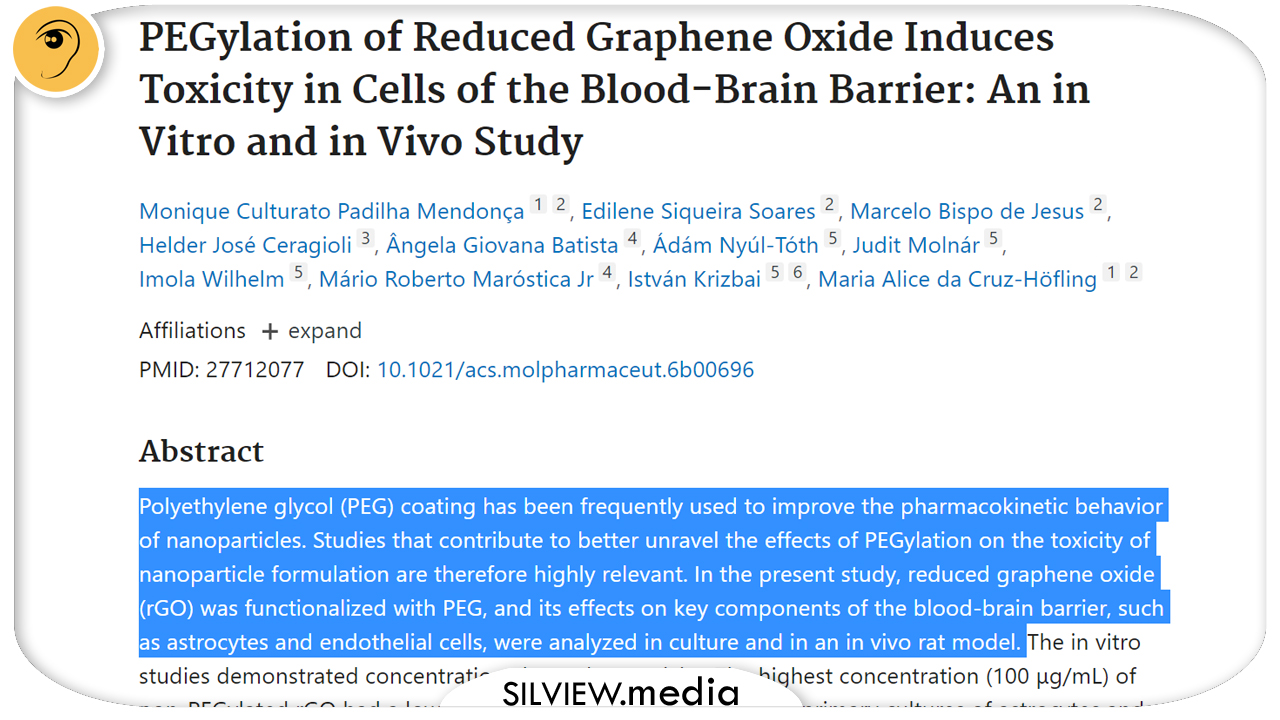
And we find out the cytoxicity is widely known inside the industry, from a very interesting invention patent that I dug out and provides excellent background information, it’s a lot, but it gives us great details as to the extent of GO usage and impact on health:
“The in vitro studies demonstrated concentration-dependent toxicity. The highest concentration (100 μg/mL) of non-PEGylated rGO had a lower toxic influence on cell viability in primary cultures of astrocytes and rat brain endothelial cells, while PEGylated rGO induced deleterious effects and cell death. We assessed hippocampal BBB integrity in vivo by evaluating astrocyte activation and the expression of the endothelial tight and adherens junctions proteins. From 1 h to 7 days post-rGO-PEG systemic injection, a notable and progressive down-regulation of protein markers of astrocytes (GFAP, connexin-43), the endothelial tight (occludin), and adherens (β-catenin) junctions and basal lamina (laminin) were observed. The formation of intracellular reactive oxygen species demonstrated by increases in the enzymatic antioxidant system in the PEGylated rGO samples was indicative of oxidative stress-mediated damage. Under the experimental conditions and design of the present study the PEGylation of rGO did not improve interaction with components of the blood-brain barrier. In contrast, the attachment of PEG to rGO induced deleterious effects in comparison with the effects caused by non-PEGylated rGO.”
Biocompatible graphene quantum dots for drug delivery and bioimaging applications – United States Patent 9642815
Abstract:
In this work we have targeted two aspects of GQDs, Size and ROS to reduce their cytotoxicity. Small size can damage cell organelles and production of ROS (reactive oxygen species) can hamper cell machinery in multiple ways. We have shown that cytotoxicity can be significantly reduced by embedding GQDs inside the PEG matrix rather than creating a thin shell around each GQD. Thin PEG shell around GQD can control ROS production but cannot circumvent the toxicity due to small size. Thus it was essential to solve both the issues. We have used a simple electrochemical method (12 h at room temperature) for synthesizing GQDs and embedded them in PEG matrix via a simple one step hydrothermal reaction (24 h at 160° C.) involving only GQDs, PEG, and deionized water. The P-GQDs formed after hydrothermal reaction show nanoparticles of diameter of ˜80-100 nm containing GQDs entrapped in PEG matrix. MTT assay showed significant 60% cells viability at a very high concentration of 5.5 mg/mL of P-GQDs compared to 10-15% viability for C-GQD and H-GQD. ROS production by P-GQDs was least compared to C-GQD and H-GQD in cell free and intracellular ROS assay suggesting involvement of ROS in cytotoxicity. In this work we have solved the issue of cytotoxicity due to ‘small size’ and ‘ROS generation’ without compromising with fluorescence properties of GQDs. P-GQDs was used for bioimaging and drug delivery in HeLa cells. In short we can obtain biocompatible P-GQDs in very short span of time with minimal use of hazardous chemicals and simple methodology.
BACKGROUND AND PRIOR ART OF THE INVENTION
A quantum dot is a semiconductor nanostructure that confines the motion of conduction band electrons, valence band holes, or excitons in all three spatial directions. Quantum dots (QDs) are traditionally chalcogenides (selenides or sulfides) of metals like cadmium or zinc (CdSe or ZnS), which range from 2 to 10 nanometers in diameter.
QDs have unique optical and electronic properties such as size-tunable light emission, narrow and symmetric emission spectra, and broad absorption spectra that enable simultaneous excitation of multiple fluorescence. Moreover, QDs are resistant to photo bleaching than organic dyes and fluorescent proteins. These properties are well suited for dynamic imaging at the single-molecule level and for multiplexed biomedical diagnostics at ultrahigh sensitivity.
However, for in vivo and clinical imaging, the potential toxicity of QDs remains a major concern. The toxic nature of cadmium-containing QDs is no longer a factor for in vitro diagnostics, since emergent use of fluorescent QDs for molecular diagnostics and pathology is an important and clinically relevant application for semiconductor QDs. (Kairdolf. B. et al., Annual Rev. of Analytical Chem. Vol. 6: 143-162.)
In prevalent practice, the use of carbon nanoparticles in synthesis of quantum dots, have emerged as a new class of quantum dot-like fluorescent nanomaterials. Carbon nanoparticles are used since their particle size can be controlled between 3-20 nm. Carbon atoms linked in hexagonal shapes, wherein each carbon atom is covalently bonded to three other carbon atoms to form graphene sheets. Graphene has the same structure of carbon atoms linked in hexagonal shapes to form carbon nanotubes, but graphene is flat rather than cylindrical.
Graphene quantum dots (GQDs) are used as fluorophores for bioimaging, owing to their physicochemical properties including tunable photoluminescence, excellent photostability, and biocompatibility. GQDs usually less than 50 nm in size have been reported to have excellent fluorescent properties. Due to luminescence stability, nanosecond lifetime, biocompatibility, low toxicity, and high water solubility, GQDs are demonstrated to be excellent probes for high contrast bioimaging and bio sensing applications.
It’s really good news that it’s become a meme topic!
References may be made to prior art documents for methods of synthesizing GQDs using electrochemical processes, hydrothermal methods and the modified Hummers process for graphene oxide synthesis and cytotoxicity assays to determine the cellular uptake of the resultant GQDs formed by these processes.
US patent publication, US 2013/0175182 provides a process for the transformation of single walled, double walled or multi walled carbon nanotubes to nanoribbons composed of few layers of graphene by a two-step electrochemical process. The process involves oxidizing dispersed carbon nanotubes (CNT) to obtain CNT oxide and further reducing it to form graphene layers.
In research publication, Chem. Commun, 2011, 6858-6860, Zhu et al, describe a method of GQD preparation wherein modified Hummers method is used for graphene oxide synthesis and hydrothermal method for GQD synthesis to obtain GQDs of particle size of 5.3 nm. At concentrations of 2.6 mg/ml, cell viability of 80% is observed.
Further Jianhua Shen et al. in New J. Chem., 2012, 36, 97-101 reported one-pot hydrothermal reaction for preparation of graphene quantum dots surface-passivated by polyethylene glycol (GQDs-PEG) and their photoelectric conversion under near-infrared light, using small graphene oxide (GO) sheets and polyethylene glycol (PEG) as starting materials.
Juan Peng et al. (Nano Lett., 2012, 12 (2), pp 844-49) describes the acid treatment and chemical exfoliation of carbon fibers, to provide GQDs in the size range of 1-4 nm. The publication provides that the GQDs derived have no toxicity at concentrations of 0.05 mg/ml. However, the cytotoxicity of GQDs at higher levels is unaccounted.
Chang Ming Li et al., (J. Mater. Chem., 2012, 8764-66) provide a method to develop graphene quantum dots (GQDs) from XC-72 carbon black by chemical oxidation, however toxicity assays confirm maximum cell viability at concentrations of 0.1 mg/ml.
The toxicity of GQDs is attributed to their size, since small sized GQDs interact with various proteins and organelles inside the cell and disrupt cellular processes. Another reason for the toxicity is their ability to generate more reactive oxygen species (ROS). Polymers, especially PEG coating has been used in the literature to decrease the toxicity of GQDs. However, even after polymer coating the cell viability at higher concentrations (>1 mg/ml) is low. Probably because even though the ROS production is lowered by the polymer shell coating, the size of the GQDs after coating still remains small (sub 50 nm) and are still in the size range that can interact with intracellular proteins and organelles.
In the following research publications, references may be made to PEGylation of carbon nanoparticles and the cell viability determined at concentrations of 1 mg/ml or lesser than that.
Bhunia et al., (Scientific Reports, 2013, 3:1473) describe carbon nanoparticles (FCN) which are polymer coated with PEG and the dosage dependent cellular toxicity of these fluorescent nanoparticles. At 1 mg/ml concentration of the FCN-PEG composition, 55-60% cell viability is observed.
Zhuang Liu et al., (J. Am. Chem. Soc., 2008, 130 (33), pp 10876-10877) describe pegylated nano-graphene oxide (NGO-PEG) of size 5-50 nm for delivery of water insoluble cancer drugs produced by Hummers method.
Omid Akhavan et al., (J. Material. Chem., 2012, Vol. 22, 20626-33) describes nontoxic concentrations of pegylated graphene nanoribbons for selective cancer cell imaging and photothermal therapy. At concentrations of 1 mg/ml of the composition. 28% cell viability was obtained.
Further Lay C L et al. (Nanotechnology. 2010 Feb. 10; 21(6):065101) reports delivery of paclitaxel by physically loading onto poly (ethylene glycol) (PEG)-graft-carbon nanotubes for potent cancer therapeutics.
Toxicity assays of GQDs synthesized by methods of the above prior arts report minimum cell viability at GQDs concentrations of 1 mg/ml, and lesser than that, thus posing limitations in cellular imaging applications. However, to realize biomedical applications of GQDs, low toxicity of the GQDS at higher concentrations is desired for cellular imaging.
With a view to provide graphene quantum dots (GQDs) with decreased cytotoxicity levels at higher concentrations i.e. greater than 1 mg/ml, the present inventors have provided a biocompatible composition of one or more graphene quantum dots (GQDs) in a nanosized polymer matrix of polyethylene glycol which is larger compared to small sized GQDs as observed in the prior art. The PEG matrix aids in reducing the reactive oxygen radicals (ROS) generated by the GQD surface while keeping the small GQDs inside the matrix; thus, also reducing their undesirable interactions with cellular proteins and organelles.
Meanwhile, these nutjobs want to use it to treat bone cancer in kids!
Or how about:
Graphene quantum dots, their composites and preparation of the same
Procedures for the synthesis of zero dimension GQDs based on exfoliation/reduction of surface passivated functionalized graphite oxide (f-GO PEG) are described. The synthesis procedures can include exfoliation/reduction f-GO PEG in presence of hydrogen gas, using focused solar radiation and under vacuum.
BACKGROUND
…
Graphene nanoribbons address this drawback of single layer graphene, however, more recently, focus has been on another carbon nanostructure called graphene quantum dots (GQDs) or carbon quantum dots (CQD) (also known as graphene quantum discs). GQDs show very desirable photoluminescence properties, as the size and shape of the GQDs can be tuned to have desired band gap and emission properties. Moreover, GQDs have desirable characteristics, for example, high surface area, larger diameter, better surface grafting using the π-π conjugated network or surface groups and other special physical properties due to the structure of graphene. Since most of the carbon nanomaterials including GQDs are biocompatible and nontoxic, GQDs can advantageously be used in biological applications for example, image scanning and sensing, drug delivery and cancer treatment. The photoluminescence properties of GQDs are useful for photovoltaic applications too as it has been theoretically proved that the energy gap in GQDs can be tuned by using electrostatic potentials.
The band gap of a GQD depends on its size and shape. With existing technology it is possible to cut graphene in to desirable size and shape forms. As the number of atoms increases, the energy gap in almost all the energy spectra of GQDs decreases monotonously. In the case of GQDs, along with size and shape, the edge type plays an important role in electronic, magnetic and optical properties.
THANKS FOR STAYING ON COURSE, THIS GOES DEEPER
This part of the article isn’t fully substantiated with third part peer-reviewed evidence, but with some of my own logic and observations, feel free to arbiter for yourself:
The graphene nano-ribbons mentioned above, if you payed attention, are most likely what La Quinta Columna and others noticed on their microscopes. Either that or carbon nanotubes, which are about the same thing, but in 3D.
Sinopeg claims it works with US scientists and collaborates with Chinese Academy. Just like Bill Gates, who is one of the very few foreign members of the Academia there, as I revealed last year. It’s almost unconceivable that Gates didn’t know of these PEGs and didn’t want to protect the secret from the general public. Sharing the manufacturing and the patents with the whole world would’ve almost certainly lead to information leaks, and that is what worried Gates more than money leaks, which are his last concern right now, I suspect.
IN CONCLUSION:
Ah, and in case you want to go even deeper into the science:
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
French citizen among six held over plan to kill Madagascar president -minister
ANTANANARIVO, July 23 (Reuters) – A French citizen is among six people arrested on suspicion of involvement in a plot to kill Madagascar’s president, the Indian Ocean island’s public security minister said, and a second official said the president’s security had been tightened.
“One of the arrested people is French, two of them are bi-national – Malagasy and French. The three others are Malagasy,” Rodellys Fanomezantsoa Randrianarison told a news conference late on Thursday.
Madagascar’s attorney general said on Thursday police had arrested the six following what officials said was a months-long investigation. read more
Patrick Rajoelina, an adviser to President Andry Rajoelina, told Reuters on Friday that two of those arrested had previously worked in the French military.
The French Foreign Affairs Ministry said it had been informed of French nationals’ arrests and that they could obtain consular help if they asked for it.
Madagascar’s President Andry Rajoelina attends a meeting to discuss the 20th replenishment of the World Bank’s International Development Association, in Abidjan, Ivory Coast July 15, 2021. REUTERS/Luc Gnago/File PhotoRead More
A spokesman for the French armed forces told Reuters he had no comment.
Patrick Rajoelina added that unspecified measures had been taken to tighten the president’s security. “The evidence is tangible and we certainly do not take this lightly,” he said.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
New from your favorite coincidence-theories magazine: There’s two timelines here that seem to meet somewhere in the recent past.
#1
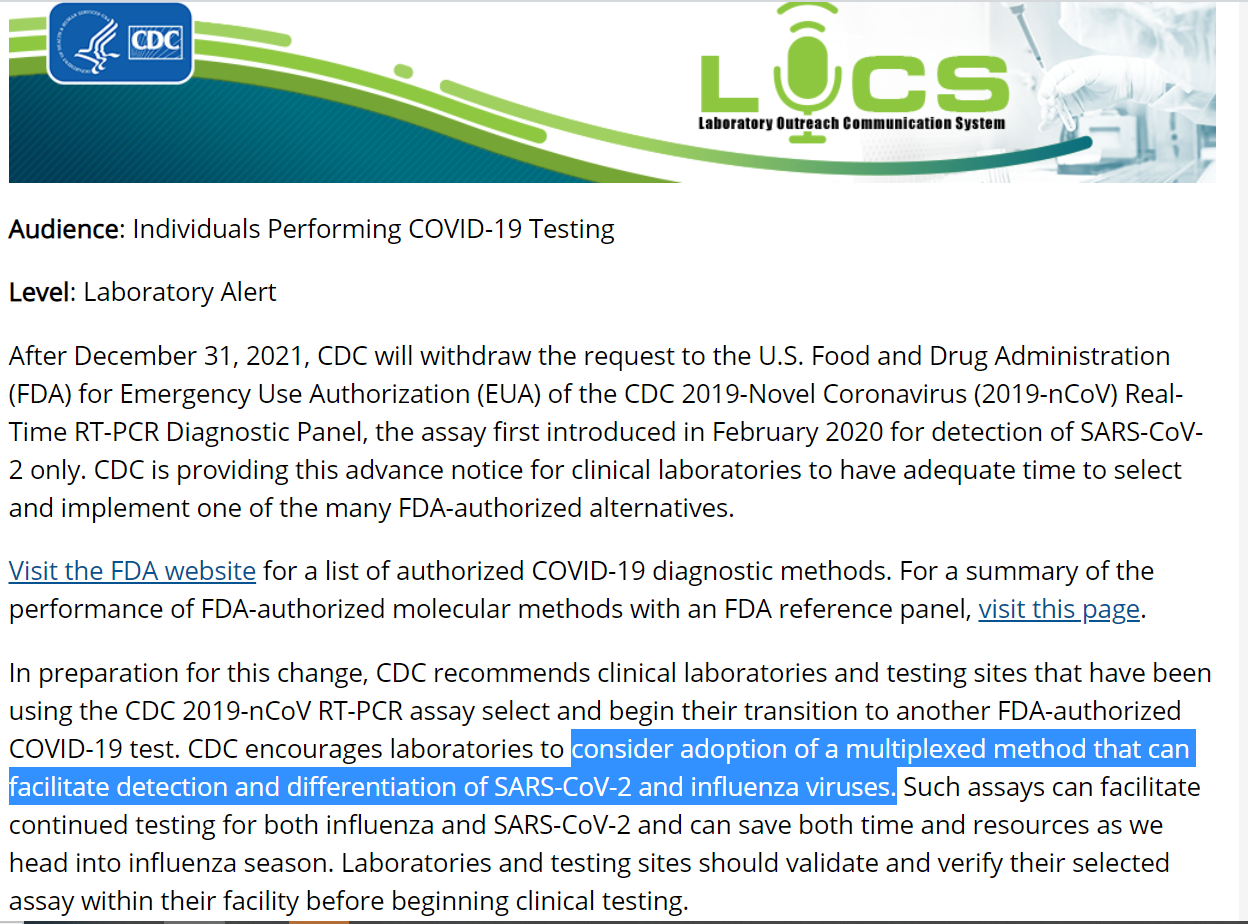
CDC has just announced retiring Covid PCR tests, starting from 2022 because they can hardly tell Covid from Flu. Where Covid is caused by a virus that no one has seen in full, purified and isolated form:
We all knew that, last summer I even made a meme where I coined the term “PCRdemic”. But just imagine how “based” their Delta Variant detection must be then! And someone was found already preparing for this, while the plebs are shocked by the admission or not even processing it.
#2
Only weeks before this announcement, media just whispered about the new unholy alliance between Soros and Gates, who suddenly decided to buy together a major UK Covid test maker.
This alliance has a legal and formal representation as the Global Access Health (GAH), something very similar to GAVI, but focused on pillaging Africa, South America and South-Asia.
Only months before this announcement, Soros and Gates became some of the most downvoted personalities in the Northern Hemisphere, with very little competition and no benefits for the public image of the Great Reset. Meanwhile, I was writing on HOW BILL GATES AND BANKSTERS GANGED UP TO TAKE MOROCCO. AND NOW ARE RUINING IT..
Only years before that, teachers and intellectuals in US were marching against Gates’ medical and food machinations in Africa.
And so forth… as far as we’re willing to dig we find ourselves entrapped and enslaved by the same inbred class that wages now a class war against the lower classes under various guises.
Every conspiratorial correlation comes with two options: conspiracy theory (causative) or coincidence theory (non-causative). I’m too experienced to hesitate here.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
This was not published for the plebs, but for their own consumption. They’ve been intoxicating themselves for quite a while, but this is one of the most striking examples I’ve seen lately. “No Means No!” As opposed to “hesitancy”.
Here’s the study, my brief critical notes come after.
COVID-19 Vaccine Hesitancy in Canada: Content Analysis of Tweets Using the Theoretical Domains Framework
Monitoring Editor: Rita Kukafka and Corey Basch Reviewed by Romaric Marcilly and Christina Cheng Janessa Griffith, BA, MSc,1,2,3 Husayn Marani, BHSc, MSc,4 and Helen Monkman, BSc, MA, PhD51
Abstract
Background
With the approval of two COVID-19 vaccines in Canada, many people feel a sense of relief, as hope is on the horizon. However, only about 75% of people in Canada plan to receive one of the vaccines.
Objective
The purpose of this study is to determine the reasons why people in Canada feel hesitant toward receiving a COVID-19 vaccine.
Methods
We screened 3915 tweets from public Twitter profiles in Canada by using the search words “vaccine” and “COVID.” The tweets that met the inclusion criteria (ie, those about COVID-19 vaccine hesitancy) were coded via content analysis. Codes were then organized into themes and interpreted by using the Theoretical Domains Framework.
Results
Overall, 605 tweets were identified as those about COVID-19 vaccine hesitancy. Vaccine hesitancy stemmed from the following themes: concerns over safety, suspicion about political or economic forces driving the COVID-19 pandemic or vaccine development, a lack of knowledge about the vaccine, antivaccine or confusing messages from authority figures, and a lack of legal liability from vaccine companies. This study also examined mistrust toward the medical industry not due to hesitancy, but due to the legacy of communities marginalized by health care institutions. These themes were categorized into the following five Theoretical Domains Framework constructs: knowledge, beliefs about consequences, environmental context and resources, social influence, and emotion.
Conclusions
With the World Health Organization stating that one of the worst threats to global health is vaccine hesitancy, it is important to have a comprehensive understanding of the reasons behind this reluctance. By using a behavioral science framework, this study adds to the emerging knowledge about vaccine hesitancy in relation to COVID-19 vaccines by analyzing public discourse in tweets in real time. Health care leaders and clinicians may use this knowledge to develop public health interventions that are responsive to the concerns of people who are hesitant to receive vaccines.
Introduction
The approval of the Pfizer-BioNTech and Moderna vaccines sent waves of excitement and relief across the world. However, some people remain hesitant about receiving a vaccine for COVID-19 [1,2]. The World Health Organization noted in 2019 that one of the greatest threats to global health was vaccine hesitancy [3]. Emerging international evidence on COVID-19 vaccine hesitancy suggests that there is a range of reasons for this reluctance, including doubts about the safety and efficacy of the vaccine, political or pharmaceutical mistrust, belief in natural immunity, and the belief that the virus is mild or not life-threatening [4–6].
For herd immunity to any communicable disease to be effective, a considerable portion of the population needs to be vaccinated or have antibodies present from being recently infected. Achieving herd immunity is difficult when a large portion of the public is not vaccinated. For herd immunity to be effective for measles and polio, 95% and 80% of the population need to be vaccinated, respectively [7]. The exact percentage required for herd immunity to COVID-19 is difficult to estimate [7].
A Statistics Canada survey conducted in September 2020 (before a vaccine was approved) indicated that 75% of Canadians were either likely or somewhat likely to receive a vaccination [8]. An Angus Reid Institute [4] study conducted between December 8 and 11, 2020 found that 48% of Canadians sampled wanted to be vaccinated immediately if a vaccine was available, and 31% wanted to be vaccinated but preferred to wait. Additionally, 7% of respondents indicated that they were unsure if they would receive a vaccination, and 14% indicated that they would not get vaccinated [4].
In the context of influenza vaccinations, there remains a broad, ethical imperative to respect others’ agency over personal health decisions (eg, choosing to not get vaccinated). However, from a public health ethics perspective, the decision to not be vaccinated creates a conflict between population safety and personal liberty [9]. As of yet, COVID-19 vaccination has not been deemed mandatory by any nation, but conversations about whether such a public mandate should exist are emerging [10]. Whether vaccines are mandated, it is worthwhile for public institutions to understand how to change behaviors concerning vaccine hesitancy to ensure that informed decision-making practices are being exercised.
Previous research has suggested that behavioral change interventions are more successful when they are grounded in theory [11]. Thus, we selected a behavioral change framework to guide this study. The Theoretical Domains Framework (TDF) was selected because of its ability to help identify the barriers and facilitators to behavior change while taking into account social and environmental factors [12]. Other public health interventions have used the TDF. For example, Garbutt et al [13] used this framework to improve human papillomavirus vaccine uptake in primary care settings. The use of such theories can facilitate the development of comprehensive health education programs [11], but this requires correctly identifying the attributes of individuals and their surroundings, which influence behavioral patterns [14]. As Bandura [15] and other behavioral theorists have posited, social norms, social relationships, and social networks have a substantial and persistent influence on behaviors [15]. It is worth understanding public discourse about vaccine hesitancy in order to develop interventions that are responsive to the needs of the population and effectively address their concerns.
In the past decade, there has been a particular interest in the utility of Twitter as a tool for monitoring and surveilling public health [16], detecting trends [17], conducting research, and disseminating information [18,19]. A systematic review of using Twitter data for health research found that most studies were in the overlapping fields of public health (23%) and infectious disease (20%) [18]. With 187 million active users worldwide as of January 2021 [20], Twitter has become a powerful social network for disseminating important public health information.
Since the start of the COVID-19 pandemic, social networking platforms like Facebook and YouTube have become stricter with their oversight of the spread of COVID-19 misinformation by deleting false information and providing hyperlinks to government websites containing credible and validated information on COVID-19. Twitter took a similar screening approach in May 2020 [21], yet the scale, spread, and speed of information sharing has made this process challenging. Further, at the start of the pandemic, Twitter introduced a system for verifying COVID-19 experts (indicated with a blue checkmark), including physicians, epidemiologists, scientists, and academics, to provide credible information concerning COVID-19 [22]. Yet, there continues to be influential individuals who have also been verified by Twitter and have enough public credibility to contradict expert opinions or present false information.
We can combat the spread of misinformation by creating targeted approaches to changing behaviors and promoting the understanding of vaccines. Thus, the purpose of this study was to identify the reasons behind vaccine hesitancy among people in Canada by conducting a content analysis of tweets through the lens of behavioral science. Our findings can be used to develop behavior change strategies and policies that are responsive to target populations.Go to:
Methods
Study Design
Twitter is a social media platform that allows users to microblog and socially network. Each user is allowed up to 280 characters in a post (called a tweet). Users can post text, pictures, videos, or links to websites. Users who have registered for an account can tweet, like, and comment on another user’s tweet and repost tweets (called a retweet). Registered users can also follow accounts and send private messages to each other. Unregistered users can read tweets, retweets, and comments but cannot engage in any interactions [23].
Twitter was selected because of its ability to capture real-time data [19]. Other studies have used Twitter to capture data on vaccine hesitancy. One study compared survey results about vaccine hesitancy in 2018 (before the COVID-19 pandemic) to data captured from Twitter and found that the data were similar to each other [24]. The study argued that Twitter could potentially be used instead of surveys in some contexts and similar results would be obtained [24]. Another study went as far as saying that Twitter is a “sentinel tool” for identifying public opinions on vaccinations [25]. Thus, Twitter was selected as the site of data collection because it offers a publicly available repository of discourse data (ie, tweets) that are captured in a specific point in time for a specific geographic area.
This study did not require research ethics approval, as it was based on data that were publicly available. Other Canadian-based studies [26] have forgone ethical review by using publicly available Twitter data, as some sources are anonymous or unidentifiable. Only the Twitter user’s username (ie, handle), city or town, and tweet content were extracted. This paper only presents aggregated data. Moreover, no interaction occurred between the authors of this study and any of the Twitter users.
Data Collection
After the researcher (JG) was approved for a developer account on Twitter, she received credentials for accessing Twitter’s application programming interface. By using a Jupyter environment, the researcher created a Python program to access Twitter’s application programming interface. Twitter allows access to tweets up to 1 week after they are posted. Thus, the researcher collected data from two time periods (December 18 and 23, 2020) to access 2 weeks’ worth of tweets. Tweets that contained the words “COVID” and “vaccine” were extracted. Similar to a library search, tweets were returned based on variations of these words, such as “COVID-19,” “COVID19,” “vaccination,” and “vaccinate.”
Data were extracted from tweets from December 10, 2020, to December 23, 2020. These dates were selected because they followed the Pfizer-BioNTech vaccine approval announcement in Canada (December 9, 2020) and included the dates for the first vaccine administration in Canada (December 14, 2020) and the approval of the Moderna vaccine in Canada (December 23, 2020). This date range also accounted for the time frame when the highest number of searches for terms that included both “COVID” and “vaccine” occurred on Google, which perhaps indicated a spike in interest [27]. Thus, our data reflects a time period when receiving a COVID-19 vaccine was close to becoming a reality. Figure 1 provides a graph that shows when data were extracted and when COVID-19–related events occurred in Canada. Figure 1 – see it in original
A graph depicting Google Trends data for the combined search terms “covid” and “vaccine” aligning with vaccine approval and administration dates in Canada. Tweets that were posted between December 10 and 23, 2020 were eligible for analysis. This date range aligned with the time when the highest peaks in related Google search activity occurred in Canada. This figure indicates that the number of searches on Google for the combined words “COVID” and “vaccine” was highest in December 9, 2020. All other searches were relative to this highest peak. For example, on December 14, 2020, roughly 70% of related searches occurred in December 9, 2020 [28]. It was not possible to obtain more detailed numbers.
To only include tweets from Canada, the researchers used five geographic radiuses that covered most of Canada. However, several small areas were unintentionally omitted (Figure 2). It was not possible to know how many tweets were missed. Figure 2 see it in original
A map of where Twitter users were located. Tweets from outside of Canada (ie, those from the United States) were excluded.
Demographic data beyond users’ locations (ie, city or town) were not collected. It was possible to obtain estimates for other demographic information, such as age and gender, from third-party companies. However, this study was operating within the confines of publicly available data so as to disseminate the findings sooner.
Data Analysis
The results were exported to a comma-separated values file and were analyzed in Microsoft Excel. Tweets were randomized (ie, reordered) in Excel so that tweets were not included based on date. As we expected, the number of tweets extracted was insurmountably high for manual analysis. Therefore, we randomly selected 20% of the tweets to be screened for eligibility. This exceeded the number of randomly selected tweets in other studies, which only included 10% of returned tweets for screening [28]. Double screening was performed for 10% of the tweets to ensure consistency. Manual analysis was selected because this study was exploratory in nature; it was unclear what themes might emerge a priori. As such, training an automated analysis program was unfeasible.
Eligible tweets included any tweets from a Canadian location that contained an expression of hesitancy toward COVID-19 vaccines. These included tweets that provided links to articles or other media that expressed hesitancy toward any COVID-19 vaccine. Eligible tweets also included those with graphics that expressed sentiments of COVID-19 vaccine hesitancy. Tweets that expressed positive or unclear sentiments toward COVID-19 vaccines were excluded. Tweets captured from the United States (given the country’s geographic proximity to Canada) were also excluded. As data were extracted on two dates, several duplicate tweets were present. These were identified and deleted in Excel.
All tweets that were deemed eligible after screening were analyzed (ie, qualitatively coded) by 2 authors (JG and HMVM). These researchers had expertise in qualitative coding. Additionally, 10% of the eligible tweets were double-coded to ensure consistency.
In Excel, a content analysis was performed on all eligible tweets. The majority of health studies that use Twitter data (56%) have conducted content analyses [18]. Content analysis was performed as described by Sutton et al [28]; the content of each tweet was systematically reviewed by at least 1 researcher. The researcher(s) then coded the content of tweets according to their meaning. The resulting codes were then organized into thematic categories. Each eligible tweet could be coded into one or more themes.
Once themes emerged from the content analysis, they were mapped onto the TDF. The TDF was selected because it applies a theory-based approach to understanding behavior and has been used extensively in implementation science research. The TDF consists of the following 14 domains: knowledge; skills; social and professional roles and identities; beliefs about capabilities; optimism; beliefs about consequences; reinforcement; intentions; goals; memory, attention, and decision processes; environmental context and resources; social influences; emotion; and behavioral regulation. It has been used in other research pertaining to seasonal flu [29] and human papillomavirus vaccine hesitancy [13] to identify barriers to vaccine uptake and plan for implementation interventions.
To these Pharma-junkies, logic sounds like The Force to an Imperial Trooper, rather used to miss the target all the time, if you catch my reference
Results
Tweet Characteristics and Themes
In total, 18,132 tweets were returned as search results. Overall, 3915 tweets were screened for eligibility. These tweets represented 21.6% of the total number of tweets. It took approximately 1 hour to manually screen 100 tweets. The 10% (400/3915) of tweets that were double-screened resulted in a Cohen κ coefficient of 0.89, indicating an almost perfect agreement. After screening, 605 tweets met the inclusion criteria. This was represented in a modified PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram (Figure 3).Figure 3
Modified PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram of the data extraction process.
Through content analysis, the included tweets were grouped into the following major themes concerning vaccine hesitancy: safety, political skepticism, influence from authority figures, a lack of knowledge, and legal liability. The final theme included medical legacies. This theme was different from the other categories of vaccine hesitancy. The themes were not mutually exclusive. Examples of tweets were not provided with the presentation of the themes to preserve the anonymity of Twitter users. In the following subsections, each theme will be described.
Safety
Overall, 48.3% (292/605) of tweets were about safety. These were largely centered around the worry that the vaccine would cause more harm than good. These tweets also expressed concerns that the COVID-19 vaccine was developed more quickly than other vaccines and that the COVID-19 vaccine was not tested to the same rigorous extent as other vaccines. Apprehension over severe side effects was also noted from tweets, including those that reported on nurses fainting and vaccine trial participants experiencing Bell palsy.
Political Skepticism
Another major theme found in 32.4% (196/605) of tweets was skepticism toward the political motivations behind vaccine development. Several Twitter users presented conspiracy theories about the COVID-19 vaccine being a vehicle for exerting political control over citizens. Other participants felt that the vaccine was not tested enough due to political pressures to reopen the economy. Several Twitter users in Canada were also highly influenced by politics in the United States; they cited rumors about the White House threatening the leadership of the US Food and Drug Administration to rush vaccine approval or face forced resignation. Tweets also indicated concern over the influence of big, government-backed pharmaceutical companies (“Big Pharma”) that were motivated by profits instead of the desire to help people.
Deficits in Medical and Epidemiologic Literacy Concerning the Benefits of Vaccination
Many tweets (159/605, 26.3%) indicated a lack of knowledge about vaccines among Twitter users. For example, several users expressed the idea that if those who contracted COVID-19 had a ≥99% survival rate, then they should not have to receive a vaccine that is said to be 95% effective. Additionally, Twitter users questioned why anyone else should be concerned if they do not receive the vaccine, indicating a lack of understanding of herd immunity. Twitter users also reported concerns about how the vaccine would alter human DNA. Several Twitter users also felt that a lack of a vaccine for cancer, heart disease, and AIDS was proof that a new virus could not be cured. Additionally, Twitter users viewed COVID-19 as a mild disease; therefore, their interest in undergoing vaccination was low.
Authority Figures
Another theme we found was mistrust toward the COVID-19 vaccine resulting from Canadian and international authority figures not taking the vaccine (51/605, 8.4%). For example, several tweets highlighted users’ mistrust toward the CEO of Pfizer and political figureheads in Canadian politics like Doug Ford (the elected provincial leader of Ontario), as they were not taking the vaccine. However, later tweets criticized public figures such as Dr Bonnie Henry (the Provincial Health Officer of British Columbia) and Alexandra Ocasio-Cortez (a member of the US House of Representatives) for receiving the vaccine before frontline workers and older adults.
Legal Liability
To a smaller extent (19/605, 3.1%), Twitter users also expressed mistrust toward vaccines that was based on reports of not being able to take legal action against drug companies if a person experiences any side effects. Additionally, news of the Federal Vaccine Injury Compensation Program in Canada resulted in further skepticism toward vaccine safety.
Medical Legacies
The final theme was unlike all of the other themes of vaccine hesitancy in this paper—the legacy of harm caused by health care institutions that have traditionally targeted the Black, Indigenous, and people of color (BIPOC) community and the lesbian, gay, bisexual, transgender, queer+ (LGBTQ+) community. Tweets (24/605, 4%) in this theme highlighted the lack of trust toward the COVID-19 vaccine resulting from how marginalized groups, such as the BIPOC and LGBTQ+ communities, have been historically targeted by the medical community. For example, the Tuskegee syphilis experiments were referenced in several tweets. Moreover, the first people who were vaccinated in the United States were Black health care workers, and several Twitter users viewed this as forced participation in medical experiments. Additionally, a poster promoting COVID-19 vaccination was viewed as paralleling the stigmatization of people who take pre-exposure prophylaxis, a medication for people living with HIV.
Theoretical Domains Framework
Themes were mapped to the TDF and categorized into the following five domains: knowledge, beliefs about consequences, environmental context and resources, social influence, and emotion. The mapping of themes to TDF domains was an interpretive and consensus-driven exercise that was conducted by two study authors (JG and HM). Disagreement was reconciled by a third study author (HMVM). Figure 4 displays a representation of the themes that were mapped to the TDF. We provide insight into this framework in the Discussion section. Overall, themes were not mutually exclusive; themes were classified according to several TDF domains. Figure 4 see it in original
Themes were categorized based on the TDF. The TDF domains are represented by the dark-gray circles. The themes from the content analysis (smaller colored circles) were mapped to relevant TDF domains. TDF: Theoretical Domains Framework.
Discussion
Principal Results
Through content analysis and TDF application, this study identified the reasons behind vaccine hesitancy among Twitter users in Canada. The major themes that emerged included concerns over safety, suspicion about political or economic forces driving the COVID-19 pandemic or vaccine development, a lack of knowledge about the COVID-19 vaccine, messages from authority figures, and a lack of legal liability from vaccine companies. An additional theme regarding the historical impact of medical mistrust among marginalized communities was also presented. These themes were categorized into the following five TDF constructs: knowledge, beliefs about consequences, environmental context and resources, social influence, and emotion. Thus, efforts to overcome vaccine hesitancy should focus on targeting these constructs.
Although evidence concerning vaccine hesitancy toward the COVID-19 vaccine is still emerging, our findings are consistent with previous studies. A study from Israel found that COVID-19 vaccine hesitancy was related to concerns about safety and efficacy and the belief that the disease is mild [5]. This was similar to our study, wherein concerns about safety was the top reason for vaccine hesitancy. The efficacy of the vaccine and the belief that the virus is mild were grouped into the lack of knowledge theme, which was another top reason for vaccine hesitancy in our study. Another study surveyed individuals from Canada and the United States in May 2020 and reported that vaccine hesitancy correlated with a lack of trust about a vaccine’s benefit, concerns about safety (ie, unknown future health consequences), commercial profiteering, and a belief in natural immunity [6]. Of note, these respondents were more likely to receive a vaccine if there was evidence of rigorous testing and safety measures [6]. Both of these studies were conducted prior to the development and implementation of a COVID-19 vaccine. As such, their results were hypothetical.
This study identified the particular reasons why people in Canada may be hesitant to receive a vaccine, so that implementation scientists who are responsible for vaccine rollouts can become responsive to these concerns. Although the analyzed tweets were from Canada, we believe that the tweets’ themes may be generalizable to other contexts. To our knowledge, no other study has analyzed tweets to determine the reasons behind COVID-19 vaccine hesitancy. This study’s contribution is especially important because the timing of our study coincided with the approval of the first two vaccines (ie, the Pfizer-BioNTech and Moderna vaccines) and the first vaccine administration in Canada.
Our results relate to vaccine hesitancy in general (ie, past research on non–COVID-19 vaccines), as prior related research has provided similar findings. For example, the influence of the media and people’s knowledge about vaccines, past experiences, perceptions of risk, and trust have all been documented [30]. However, hesitancy toward the COVID-19 vaccines presents new, unprecedented challenges; namely, the global COVID-19 pandemic is unlike any pandemic that has been experienced in the past century, herd immunity depends on vaccine participation on a global scale, and new SARS-CoV-2 strains can emerge if the virus has opportunities (ie, time and vectors) to mutate. Additionally, the long-term health consequences of COVID-19 are unknown [31].
Our recommendation for the organizations responsible for implementing vaccination programs is to create behavioral interventions that are responsive to the concerns presented in this study. The mapping of these themes to the TDF provided us with preliminary insights into how to best target these behavioral interventions. For example, safety was a top concern that was found in the tweets, and we mapped safety to both knowledge and beliefs about consequences. Thus, targeting vaccine literacy may be beneficial, and this can be done by explaining how vaccines work, why they are safe, and how no steps were missed in the expedient process of COVID-19 vaccine development. However, trust in politicians and pharmaceutical companies is a vaccine hesitancy factor that is difficult to target because both groups are necessarily involved in vaccine rollouts. One approach to targeting this concern might be to have trusted physicians speak to their patients about why it is important to be immunized. This approach falls under the domain of emotion in the TDF.
Although providing details on interventions for responding to vaccine hesitancy was beyond the scope of this study, Table 1 provides example suggestions for interventions based on each TDF domain.
Table 1
Reasons for vaccine hesitation fell under several Theoretical Domains Framework (TDF) constructs (left column). The rightmost column provides examples of intervention suggestions for responding to vaccine hesitancy in relation to the TDF construct.
TDF constructs
Content analysis theme
Example suggestions
Knowledge
Lack of knowledge
Introduce campaigns that educate the public about using clear language in media that are commonly used to digest content (eg, social media).
Social influence
Authority
Have nonpolitical, respected older adult Canadian celebrities take the vaccine as an example. Such celebrities could be retired athletes or musicians.
Environmental context and resources
Political skepticism
Emphasize that vaccines are rooted in science and not politics. This is a difficult quality to understand.In action, this could be done by having messages come from trusted physicians instead of politicians.
Emotion and beliefs about consequences
Safety
Highlight examples of instances when the vaccine has worked.Reiterate the safety of the vaccine.Reiterate the fact that the steps in the scientific development of the vaccine were not missed.
More research is necessary to determine whether addressing these concerns is effective in overcoming vaccine hesitancy.
Limitations
As of January 2021, roughly 6.45 million (~17%) Canadians use Twitter [32]. Therefore, the perspectives on vaccine hesitancy presented in this paper are not wholly representative of the perspectives of all people in Canada. All users included in this study represent people in Canada with broadband internet access, which, as the COVID-19 pandemic has illustrated, is an important determinant of health [33]. As such, we likely missed the perspectives of those who face challenges when accessing the internet. It is also possible that nonhuman Twitter users (bots) were represented in our sample. Previous research has found that Twitter bots have manipulated public opinion and fueled cascades of negative emotions related to topics about COVID-19 [34]. Without any way to systematically identify and exclude these tweets, we suspect that several such tweets were included in our analysis. We also searched for English-only tweets due to limitations in language expertise among this study’s authors. A more comprehensive content analysis that is representative of all people in Canada should include tweets that are written in other languages. This limitation may have resulted in themes not being identified, including those related to culturally specific concerns.
It was not possible to collect demographic data such as age, gender, and ethnicity while also preserving users’ anonymity. Thus, we were unable to analyze the demographic characteristics of Twitter users who expressed vaccine hesitancy.
Although the search strategy could have been expanded to include many more terms related to vaccination (eg, “shot,” “jab,” “immunization,” etc), the search results would have been insurmountable for conducting our manual analysis process. Additionally, terms related to hoax beliefs were not included; the inclusion of such terms would have likely produced more results. Although saturation was achieved for our search, we may have missed themes that used alternative language to express vaccine hesitancy.
Of note, the examples of interventions presented in Table 1 are merely suggestions. A behavioral scientist may have more informed suggestions about how to combat vaccine hesitancy according to the TDF.
Finally, the tweets related to the medical legacies discussed in this paper should not be viewed as tweets about vaccine hesitancy or conflated with those under the categories of safety, a lack of knowledge, political skepticism, messages from authority figures, and legal liability. As Mosby and Sridrovich [35] have emphasized, health care providers need to understand the history of “racially segregated health care and medical experimentation.” Additionally, Boyd [36] stated that the “hyper-focus on hesitancy implicitly blames Black communities for their undervaccination, and it obscures opportunities to address the primary barrier to COVID-19 vaccination: access.” Building trust in the medical system goes far beyond the suggestions presented in this paper.
Conclusions
Overall, this study identified the reasons why people in Canada may feel hesitant toward receiving a COVID-19 vaccine. These reasons fell under the following themes: safety concerns, suspicions about political or economic forces, a lack of knowledge, messages from authority figures, and a lack of legal liability from vaccine companies. Additionally, other tweets revealed the historical impact of medical mistrust among marginalized communities, which should not be viewed as hesitancy or as the result of the reasons identified in this paper. Overall, behavioral, implementation, and public health scientists can use theory-based approaches like the TDF to design interventions that are tailored to address the concerns that people have and improve the uptake of the COVID-19 vaccine, thereby increasing the chances of achieving the threshold necessary for herd immunity.Go to:
Acknowledgments
JG conceived the study idea and was involved in all study activities, including study data extraction and analysis and manuscript preparation. HM supported the literature extraction and manuscript preparation. HMVM supported the coding of tweets and manuscript revision. This study was conducted without financial support.Go to:
Abbreviations
BIPOC
Black, Indigenous, and people of color
LGBTQ+
lesbian, gay, bisexual, transgender, queer+
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
TDF
Theoretical Domains Framework
Footnotes
Conflicts of Interest: None declared.
LIVE FROM THE TRENCHES, Here’s just a few of the many reasons this is trash and whoever takes it seriously is a self-deluded clown:
There’s almost no hesitancy in 2021. Whoever was hesitant before, stopped being so in 2020. Same way many of us stopped hesitating on 9/11. If they are not favorable, most of the messages out there are anti-certainly-harmful-covid-injections. Most of us don’t even think of them as “vaccines”. By a large.
As opposed to the people they studied, Pharmafia self-intoxicates itself lumping Covid injections with vaccines. But the two draw support from different crowds. Which leads to the next self-intoxication:
There’s new categories that their radar doesn’t even have sensors for: general pro-vaxxers who are either hesitant or determined not to take covid injections, as they keep taking vaccines. And the hesitant fraction of the fraction is tiny.
Twitter is filled with pharmabots who infiltrate anti-vaxx communities. Thus, Pharmafia did a Hunter Biden again, and fell asleep with a meth pipe still hot between the upper lips. That was for sale. Besides that, it’s been shown that Twitter is the least accurate reflection of the general population of all social media networks, so the flaw is embedded in the pool.
“Many tweets (159/605, 26.3%) indicated a lack of knowledge about vaccines among Twitter users” – Where does “many” start, that’s actually only a quarter, very little compared to how they portrait anti-vaxxers as generally Neanderthals. Also very little compared to pro-vaxx scores, where medical illiteracy is predominant even when they’re ideologically aligned with Pharmafia. A minimal intellectual decency requires a bit of comparative study there on the literacy – vaccine-opposition correlation. Or causation. But their main problem here is that they lump together ignoramus and people unaligned with the official lies exactly because they are in the know. The two don’t respond the same to whatever you want to do to them. Pharmafia’s gonna have a bad time if it keeps swallowing its own baits, can’t wait for the next laugh from them. I mean how much BS can you pack in a single sentence in a self-served “scientific” work? How is this any healthier than meth?
There’s a huge mindset difference between someone who understood the truth and stopped hesitating and someone who’s in the process and still hesitating. Much larger than the difference between “anti-certainly-harmful-covid-injections” and “vaccine-hesitant”. Respectively, once you know, you can’t unknow. Once you left the womb, you can’t go back to be fed through an umbilical cord. So they only have a chance at people who don’t know enough yet and they can only hope to prevent them from getting there. But Pharmafia is guaranteed to fail as it keeps consuming the propaganda stash it fabricated for sale.
I wrote this mainly so we can mock them again later and shout “Told you so, dum’asses!’
PS: Isn’t “The Journal of Internet Medical Research” doing exactly what anti-vaxxers were mocked for with those “Google diplomas” 0IQ jokes?
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Every time I hear Pharma dispensers like Paul Ofitt or Pharma trolls like Biden accusing non-vaccinated people of murder, this study comes to mind first thing. This British Medical Journal analysis used to be one of the first shadow-banned links on Facebook, years before the term was even coined. Together with Google, they managed to fade it out from public attention and references, but it’s a staple of medical journalism and criticism.
Medical error—the third leading cause of death in the US
Summary points -Death certificates in the US, used to compile national statistics, have no facility for acknowledging medical error -If medical error was a disease, it would rank as the third leading cause of death in the US -The system for measuring national vital statistics should be revised to facilitate better understanding of deaths due to medical care
Medical error is not included on death certificates or in rankings of cause of death. Martin Makary and Michael Daniel assess its contribution to mortality and call for better reporting
The annual list of the most common causes of death in the United States, compiled by the Centers for Disease Control and Prevention (CDC), informs public awareness and national research priorities each year. The list is created using death certificates filled out by physicians, funeral directors, medical examiners, and coroners. However, a major limitation of the death certificate is that it relies on assigning an International Classification of Disease (ICD) code to the cause of death.1 As a result, causes of death not associated with an ICD code, such as human and system factors, are not captured. The science of safety has matured to describe how communication breakdowns, diagnostic errors, poor judgment, and inadequate skill can directly result in patient harm and death. We analyzed the scientific literature on medical error to identify its contribution to US deaths in relation to causes listed by the CDC.2
Death from medical care itself
Medical error has been defined as an unintended act (either of omission or commission) or one that does not achieve its intended outcome,3 the failure of a planned action to be completed as intended (an error of execution), the use of a wrong plan to achieve an aim (an error of planning),4 or a deviation from the process of care that may or may not cause harm to the patient.5 Patient harm from medical error can occur at the individual or system level. The taxonomy of errors is expanding to better categorize preventable factors and events.6 We focus on preventable lethal events to highlight the scale of potential for improvement.
Case history: role of medical error in patient death A young woman recovered well after a successful transplant operation. However, she was readmitted for non-specific complaints that were evaluated with extensive tests, some of which were unnecessary, including a pericardiocentesis. She was discharged but came back to the hospital days later with intra-abdominal hemorrhage and cardiopulmonary arrest. An autopsy revealed that the needle inserted during the pericardiocentesis grazed the liver causing a pseudoaneurysm that resulted in subsequent rupture and death. The death certificate listed the cause of death as cardiovascular.
The role of error can be complex. While many errors are non-consequential, an error can end the life of someone with a long life expectancy or accelerate an imminent death. The case in the box shows how error can contribute to death. Moving away from a requirement that only reasons for death with an ICD code can be used on death certificates could better inform healthcare research and awareness priorities.
How big is the problem?
The most commonly cited estimate of annual deaths from medical error in the US—a 1999 Institute of Medicine (IOM) report7—is limited and outdated. The report describes an incidence of 44 000-98 000 deaths annually.7 This conclusion was not based on primary research conducted by the institute but on the 1984 Harvard Medical Practice Study and the 1992 Utah and Colorado Study.8 9 But as early as 1993, Leape, a chief investigator in the 1984 Harvard study, published an article arguing that the study’s estimate was too low, contending that 78% rather than 51% of the 180 000 iatrogenic deaths were preventable (some argue that all iatrogenic deaths are preventable).10 This higher incidence (about 140 400 deaths due to error) has been supported by subsequent studies which suggest that the 1999 IOM report underestimates the magnitude of the problem. A 2004 report of inpatient deaths associated with the Agency for Healthcare Quality and Research Patient Safety Indicators in the Medicare population estimated that 575 000 deaths were caused by medical error between 2000 and 2002, which is about 195 000 deaths a year (table 1⇓).11 Similarly, the US Department of Health and Human Services Office of the Inspector General examining the health records of hospital inpatients in 2008, reported 180 000 deaths due to medical error a year among Medicare beneficiaries alone.12 Using similar methods, Classen et al described a rate of 1.13%.13 If this rate is applied to all registered US hospital admissions in 201315 it translates to over 400 000 deaths a year, more than four times the IOM estimate. Similarly, Landrigan et al reported that 0.6% of hospital admissions in a group of North Carolina hospitals over six years (2002-07) resulted in lethal adverse events and conservatively estimated that 63% were due to medical errors.14 Extrapolated nationally, this would translate into 134 581 inpatient deaths a year from poor inpatient care. Of note, none of the studies captured deaths outside inpatient care—those resulting from errors in care at home or in nursing homes and in outpatient care such as ambulatory surgery centers.
A literature review by James estimated preventable adverse events using a weighted analysis and described an incidence range of 210 000-400 000 deaths a year associated with medical errors among hospital patients.16 We calculated a mean rate of death from medical error of 251 454 a year using the studies reported since the 1999 IOM report and extrapolating to the total number of US hospital admissions in 2013. We believe this understates the true incidence of death due to medical error because the studies cited rely on errors extractable in documented health records and include only inpatient deaths. Although the assumptions made in extrapolating study data to the broader US population may limit the accuracy of our figure, the absence of national data highlights the need for systematic measurement of the problem. Comparing our estimate to CDC rankings suggests that medical error is the third most common cause of death in the US (fig 1⇓).2
Better data
Human error is inevitable. Although we cannot eliminate human error, we can better measure the problem to design safersystems mitigating its frequency, visibility, and consequences. Strategies to reduce death from medical care should include three steps: making errors more visible when they occur so their effects can be intercepted; having remedies at hand to rescue patients 17; and making errors less frequent by following principles that take human limitations into account (fig 2⇓). This multitier approach necessitates guidance from reliable data. Currently, deaths caused by errors are unmeasured and discussions about prevention occur in limited and confidential forums, such as a hospital’s internal root cause analysis committee or a department’s morbidity and mortality conference. These forums review only a fraction of detected adverse events and the lessons learnt are not disseminated beyond the institution or department. There are several possible strategies to estimate accurate national statistics for death due to medical error. Instead of simply requiring cause of death, death certificates could contain an extra field asking whether a preventable complication stemming from the patient’s medical care contributed to the death. An early experience asking physicians to comment on the potential preventability of inpatient deaths immediately after they occurred resulted in an 89% response rate.18 Another strategy would be for hospitals to carry out a rapid and efficient independent investigation into deaths to determine the potential contribution of error. A root cause analysis approach would enable local learning while using medicolegal protections to maintain anonymity. Standardized data collection and reporting processes are needed to build up an accurate national picture of the problem. Measuring the consequences of medical care on patient outcomes is an important prerequisite to creating a culture of learning from our mistakes, thereby advancing the science of safety and moving us closer towards the Institute of Medicine’s goal of creating learning health systems. (19)
Health priorities
We have estimated that medical error is the third biggest cause of death in the US and therefore requires greater attention. Medical error leading to patient death is under-recognized in many other countries, including the UK and Canada.20 21 According to WHO, 117 countries code their mortality statistics using the ICD system as the primary indicator of health status.22 The ICD-10 coding system has limited ability to capture most types of medical error. At best, there are only a few codes where the role of error can be inferred, such as the code for anticoagulation causing adverse effects and the code for overdose events. When a medical error results in death, both the physiological cause of the death and the related problem with delivery of care should be captured. To achieve more reliable healthcare systems, the science of improving safety should benefit from sharing data nationally and internationally, in the same way as clinicians share research and innovation about coronary artery disease, melanoma, and influenza. Sound scientific methods, beginning with an assessment of the problem, are critical to approaching any health threat to patients. The problem of medical error should not be exempt from this scientific approach. More appropriate recognition of the role of medical error in patient death could heighten awareness and guide both collaborations and capital investments in research and prevention. Contributors and sources: MM is the developer of the operating room checklist, the precursor to the WHO surgery checklist. He is a surgical oncologist at Johns Hopkins and author of Unaccountable, a book about transparency in healthcare. MD is the Rodda patient safety research fellow at Johns Hopkins and is focused on health services research. This article arose from discussions about the paucity of funding available to support quality and safety research relative to other causes of death.
1 Moriyama IM, Loy RM, Robb-Smith AHT, et al. History of the statistical classification of diseases and causes of death. National Center for Health Statistics, 2011. 2 Deaths: final data for 2013. National vital statistics report. http://www.cdc.gov/nchs/fastats/ leading-causes-of-death.htm. 3 Leape LL. Error in medicine. JAMA 1994;272:1851-7. doi:10.1001/jama.1994. 03520230061039 pmid:7503827. 4 Reason J. Human error. Cambridge University Press, 1990. doi:10.1017/ CBO9781139062367. 5 Reason JT. Understanding adverse events: the human factor. In: Vincent C, ed. Clinical risk management: enhancing patient safety. BMJ, 2001:9-30. 6 Grober ED, Bohnen JM. Defining medical error. Can J Surg 2005;48:39-44.pmid:15757035. 7 Kohn LT, Corrigan JM, Donaldson MS. To err is human: building a safer health system. National Academies Press, 1999. 8 Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med 1991;324:370-6. doi:10.1056/NEJM199102073240604 pmid:1987460. 9 Thomas EJ, Studdert DM, Newhouse JP, et al. Costs of medical injuries in Utah and Colorado. Inquiry 1999;36:255-64.pmid:10570659. 10 Leape LL, Lawthers AG, Brennan TA, Johnson WG. Preventing medical injury. Qual Rev Bull 1993;19:144-9.pmid:8332330. 11 HealthGrades quality study: patient safety in American hospitals. 2004. http://www. providersedge.com/ehdocs/ehr_articles/Patient_Safety_in_American_Hospitals-2004.pdf. 12 Department of Health and Human Services. Adverse events in hospitals: national incidence among Medicare beneficiaries. 2010. http://oig.hhs.gov/oei/reports/oei-06-09-00090.pdf. 13 Classen D, Resar R, Griffin F, et al. Global “trigger tool” shows that adverse events in hospitals may be ten times greater than previously measured. Health Aff 2011;30:581-9doi: 10.1377/hlthaff.2011.0190. 14 Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med 2010;363:2124-34. doi:10.1056/NEJMsa1004404 pmid:21105794. 15 American Hospital Association. Fast facts on US hospitals. 2015.http://www.aha.org/ research/rc/stat-studies/fast-facts.shtml. 16 James JTA. A new, evidence-based estimate of patient harms associated with hospital care. J Patient Saf 2013;9:122-8. doi:10.1097/PTS.0b013e3182948a69 pmid:23860193. 17 Ghaferi AA, Birkmeyer JD, Dimick JB. Complications, failure to rescue, and mortality with major inpatient surgery in Medicare patients. Ann Surg 2009;250:1029-34. doi:10.1097/ SLA.0b013e3181bef697 pmid:19953723. 18 Provenzano A, Rohan S, Trevejo E, Burdick E, Lipsitz S, Kachalia A. Evaluating inpatient mortality: a new electronic review process that gathers information from front-line providers. BMJ Qual Saf 2015;24:31-7. doi:10.1136/bmjqs-2014-003120 pmid:25332203. 19 Institute of Medicine of the National Academies. Continuous improvement and innovation in health and health care. Round table on value and science-driven health care. National Academies Press, 2011. 20 Office for National Statistics’ Death Certification Advisory Group. Guidance for doctors completing medical certificates of cause of death in England and Wales. 2010. 21 Statistics Canada. Canadian vital statistics, death database and population estimates. http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/hlth36a-eng.htm. 22 World Health Organization. International classification of diseases.http://www.who.int/ classifications/icd/en/.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
If you’re a typical millennial, schooled, not educated, and with no historical time perception, you may think this happened ages ago and it’s no longer relevant. But the victims would be younger than my mom today and the affair has been concluded just a few years before my birth. It is conceivable that some of the participants are still working and giving advice on Covid nowadays.
Pharmafia and its faucist lemmings have jumped on an imaginary flying white horse and are pointing fingers at all dissatisfied costumers and skeptics from some imaginary moral heights they fly in their empathy-deficient heads. They call out racism, egoism and what not in everyone who’s not a Pharma-junkie yet, projecting their own faults all over the place like a garden sprinkler made by Goebbels Industries . They need bitch-slapped back into reality with some historical facts. Because if a person had Pharmafia’s criminal record, you’d ask for bodyguards and a restraining order, and the last thing you’d take from them would be health-advice.
THE HIDDEOUS THRUTHS OF TESTING VACCINES ON HUMANS
Sixty years ago, a monstrous hepatitis experiment was performed on mentally disabled children at Willowbrook State School that raises serious ethical questions about vaccine challenge trials for Covid-19.
Nina Galen was ten years old when she became part of one of the most controversial human experiments in American history. Her mother, Diana McCourt, was looking for an institution that could care for her severely autistic daughter. “I was just desperate,” McCourt says now, more than 50 years later. “I think I was having a breakdown because I was just trying to take care of everything.”
McCourt finally settled on Willowbrook State School, a home for severely developmentally challenged children and adults on Staten Island, New York. In order to get Nina a spot at the overcrowded facility, however, she had to make a Faustian bargain—consenting to allow her daughter to be part of a quest to find a vaccine for hepatitis. “I had no choice,” McCourt says, “I had tried so many different places and so many arrangements, and they didn’t work out, so I went along with it.”
Nina became one of more than 50 mentally disabled children, ages 5 to 10, under the care of Dr. Saul Krugman, a respected pediatrician from New York who wanted to determine if there were multiple strains of hepatitis, and whether a vaccine could be created to protect against the disease. Krugman and his partner, Dr. Joan Giles, used the Willowbrook residents to test a preliminary vaccine for this disease that had killed millions worldwide. From 1955 to 1970, the children were injected with the virus itself or made to drink chocolate milk mixed with feces from other infected children in order to study their immunity.
For much of human history, hepatitis caused some of the deadliest outbreaks in the world. The symptoms, including fever, liver damage and yellow skin, were written about by Hippocrates in the fifth century B.C.E. While we now know that there are multiple viruses (most famously, hepatitis A, B and C), in the first half of the 20th century researchers only knew of one form of the disease, which was then called epidemic jaundice.
Finding a vaccine became particularly important for the United States during World War II, when hepatitis outbreaks affected more than 50,000 American troops. To fight this disease and others, the Surgeon General’s office established the Armed Forces Epidemiological Board.
School for Scandal: In addition to conducting hepatitis experiments, Willowbrook’s staff physically abused residents.
In the early 1950s, Dr. Krugman, a former flight surgeon for the U.S. Army Air Corps, went to the Epidemiological Board with a proposition: he wanted to create a vaccine for hepatitis, and knew the perfect place where he could do his research. Willowbrook was overcrowded, already rampant with disease, and at the time it wasn’t uncommon to test vaccines on children.
The idea goes back to the grandfather of vaccines himself, Edward Jenner, who used an 8-year-old boy as the first test subject of his groundbreaking smallpox vaccine in the late 18th century. The Willowbrook hepatitis experiments would be vaccine challenge experiments, so-called because the body is intentionally “challenged” with a direct exposure to the virus to see if a particular treatment prevents someone from getting the disease.
“He believed he was helping the children at this school deal with the epidemic,” says Dr. Krugman’s son Richard, a pediatrician at the Children’s Hospital Colorado and former head of the U.S. Advisory Board on Child Abuse and Neglect. “He certainly thought he was making a contribution to infectious disease research.”
Although there’s little doubt that Dr. Krugman accelerated the discovery of a hepatitis vaccine, the ethics of his experiment have resurfaced as vaccine challenge trials are being debated for Covid-19. Many politicians, medical ethicists and scientists have come out in favor of the idea, which would include giving healthy volunteers a dose of an unproven vaccine, and then deliberately exposing them to Covid-19 to see if it offers protection against the virus.
While the vaccine challenge trials would be done with healthy adult volunteers, the Covid-19 vaccine challenge trial and the Willowbrook hepatitis experiments beg the same question: Is it really necessary—or right—to risk the health of a few for the benefit of many?
Saul Krugman arrived at the bucolic Willowbrook campus in 1955. Nestled on almost 400 acres on Staten Island, the large, U-shaped brick buildings were surrounded by a lush green forest. A painted yellow and blue carousel sat at the entrance to the grounds, and first-time visitors described it as enchanting, like a summer camp. Inside, however, Willowbrook was a nightmare.
Do No Harm: RFK described Willowbrook’s conditions as “less comfortable and cheerful than the cages in which we put animals in a zoo.” But since the kids were mostly white and many of the “caregivers” black, I doubt libtards will get triggered by this
The school opened in 1947 and was built to hold 4,000 residents, but for years that number was over 6,000. Disease and neglect were everywhere, and multiple residents died from untreated illness and abuse. In 1965, Robert F. Kennedy, then a New York Senator, made an unannounced visit to Willowbrook and left appalled. “There are no civil liberties for those put in the cells of Willowbrook,” he later testified before Congress, calling the institution a “snake pit.”
When Dr. Krugman and Dr. Giles began the Willowbrook hepatitis experiments, they used the conditions of Willowbrook to their advantage for recruiting new families. Despite its well-documented horrors, Willowbrook was still one of the only options for children with severe disabilities, and there was a long waitlist. Dr. Krugman offered several parents, including Nina Galen’s, the ability to jump the line and have their children put in the newer, cleaner research wards with more staff—if they joined the experiments. “I did feel coerced,” McCourt says, “I felt like I was denied help unless I took this [opportunity].”
Krugman also told parents that since hepatitis was already prevalent at Willowbrook, their children may as well have the chance for a vaccine. McCourt remembers being told her daughter could get an “antidote” to hepatitis if she joined the experiment. When she asked why the hepatitis studies couldn’t be done on primates, she was told that using animals would be “too expensive.”
Despite understanding the optics of infecting mentally disabled children with a potentially deadly disease, Dr. Krugman felt the risk was worth the reward. “The decision to feed hepatitis virus to patients at Willowbrook was not undertaken lightly,” he wrote in a 1958 paper published in the New England Journal of Medicine. He noted that the strain of hepatitis in Willowbrook wasn’t very severe, that many of the children would get infected anyway, and that any knowledge gained from the experiment would in fact help other Willowbrook residents. He also emphasized that the study was sanctioned by the New York State Department of Mental Hygiene, and the Armed Forces Epidemiological Board of the Surgeon General’s Office.
“I don’t think you’re ever justified to inoculate a child with an infectious virus that might kill them,” says pediatrician Paul Offit.
Some of Dr. Krugman’s trials built on previous research that giving children antibodies from patients who had recovered from hepatitis could prevent new infections. (A similar concept, using convalescent plasma of recovered Covid-19 patients to treat sick patients, is being explored today.)
The experiments also involved infecting healthy children with the virus through the chocolate milk concoction. The doctors eventually learned how much it took for the children to show symptoms of hepatitis, allowed them to recover, and then gave them the virus all over again. These experiments were done to test if someone who had recovered from hepatitis would remain immune or if they could be reinfected again.
As each trial concluded, Dr. Krugman published the results in prominent medical journals including the New England Journal of Medicine, the Lancet, and the Journal of the American Medical Association. From the time of the first publication, the experiments were controversial within the medical community. In 1966, renowned medical ethicist Henry K. Beecher published an article titled, “Ethics and Clinical Research,” which listed Willowbrook as an example of an unethical clinical experiment and concluded that “there is no right to risk an injury to one person for the benefit of others.”
Five years later, the editorial board of the Lancet apologized for publishing Dr. Krugman’s studies without greater skepticism. “The Willowbrook experiments have always carried a hope that hepatitis might one day be prevented,” the editors wrote, “but that could not justify the giving of infected material to children who would not directly benefit.” A year later, Krugman had to ward off protesters at a medical conference in Atlantic City.
Bad Form: Willowbrook often accepted children in exchange for parental permission to conduct hepatitis testing. THE COLLEGE OF STATEN ISLAND ARCHIVES AND SPECIAL COLLECTIONS
“I think he got a lot of flak for it from people who didn’t understand the context or the reality of the institution,” Richard Krugman says. “It certainly got caught up in the politics of the day.”
But Dr. Krugman had as many fans as he did detractors. New York State Senator Seymour Thaler, originally a critic of the hepatitis experiments, later said that Krugman had “done a magnificent thing.” Dr. Franz Ingelfinger, a former editor of the New England Journal of Medicine, also supported the research. “How much better to have a patient with hepatitis, accidentally or deliberately acquired, under the guidance of a Krugman than under the care of a zealot,” he wrote.
In addition to discovering the hepatitis A and B strains, Dr. Krugman “certainly did speed up the development of a hepatitis B vaccine,” says Paul Offit, a pediatrician and director of the Vaccine Education Center at The Children’s Hospital of Philadelphia. But, Offit adds, “I don’t think you’re ever justified to inoculate a child with an infectious virus that might kill them.”
As members of the medical community protested Krugman’s experiments, a greater force was mobilizing to close down Willowbrook for good.
In 1972, Geraldo Rivera, then a local television reporter in New York, snuck into the grounds of the school and broadcast the inhumane conditions of Willowbrook. He had been tipped off about the residents’ living conditions by Michael Wilkins, a doctor at the school who was not involved in the hepatitis trials.
“It’s almost 50 years and speaking about it still makes me cry,” says Rivera, now a roaming correspondent-at-large at Fox News. “The conditions were so horrible.” Rivera remembers seeing children naked, smeared in their own feces and hitting their heads against the wall. “I would imagine that the situation I had was similar to the GIs that freed the concentration camps.”
The Last Great Disgrace: As a result of Geraldo Rivera’s 1972 investigation of Willowbrook, a federal law was passed to protect people in institutions. MICHAEL OCHS/ GETTYIMAGES
At roughly the same time, a whistleblower exposed the infamous Tuskegee syphilis study in which researchers deliberately let hundreds of Black men go untreated and several died from the disease, even though there was a known cure. Willowbrook was one in a long line of human experimentations on children, prison inmates, people in mental health facilities, and minority communities, and Tuskegee was the tipping point.
Dr. Krugman, however, was rewarded for his work at Willowbrook. That year, he became president of the American Pediatric Society.
In 1974, the National Research Act was passed in an effort to create regulations that protected subjects in human research trials. One measure it implemented was the creation of an ethics task force, the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. “The National Commission might never have come into being were it not for Willowbrook and Tuskegee and several other instances,” says Karen Lebacqz, one of the original members of the commission.
By 1979 the commission had published the Belmont Report, a comprehensive guideline of basic ethical principles that guide modern clinical trials. The National Research Act also established the practice of Institutional Review Boards (IRBs), independent committees that must take time to review the ethical aspects of human clinical trials to this day.
Aside from potential ethical dilemmas, today’s coronavirus vaccine challenge trials have something else in common with the Willowbrook hepatitis experiments: they may not even be necessary. While Dr. Krugman is credited for speeding up the development of a hepatitis vaccine, other researchers were not far behind. In the late 1960s, Dr. Baruch Blumberg independently discovered the hepatitis B virus, and together with Dr. Irving Millman submitted the first patent for a hepatitis vaccine in 1969. Blumberg did all his research by taking blood samples and testing the liver functions on children and adults who were already infected, and his work earned Blumberg a Nobel Prize for Medicine.
“Whenever people are desperate,” ethics professor Karen Lebacqz says, “they always want to relax ethical standards.”
Similarly, even if a challenge trial for coronavirus gets approved, there’s no guarantee that it will lead to a faster vaccine development. The U.S. government’s initiative to develop a coronavirus vaccine may be called “Operation Warp Speed,” but Christine Grady, Chief of the Department of Bioethics at the National Institutes of Health Clinical Center, says that a lot of time and thought have to be put into properly designing a trial.
“Whether or not doing a challenge trial would even speed up the trial is a question that is not exactly clear,” says Grady, who is married to Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases. Paul Offit agrees. “You have to have the right dose. And to get the right dose, you have to have these mini-challenge trials,” he says. “I don’t think it’s going to happen.”
Karen Lebacqz, one of the original Belmont Report authors, also has concerns about the accelerated Covid-19 vaccine protocols. “Whenever people are desperate,” she says, “they always want to relax ethical standards.”
Saul Krugman’s controversial experiments at Willowbrook were only the beginning of his illustrious career. He later became the head of pediatrics at New York University School of Medicine, was elected to the National Academy of Sciences, authored a classic textbook of pediatric infectious diseases, received the prestigious Lasker Award, and helped to develop the first rubella and measles vaccines.
He defended the Willowbrook trials his whole life, writing in 1986, “I am as convinced today as I was at that time that our studies were ethical and justifiable.” Krugman passed away in 1995, and his obituary in the New York Times has only a small mention of his experiments at Willowbrook.
To this day, while many modern-day ethicists use the Willowbrook studies as an example of unjust human experimentation, there are always second opinions. “It’s complicated,” Grady says. To her knowledge, “Krugman’s first goal was to understand the disease…but I think there are some things about it that certainly don’t look good and would be hard to get approval today.”
Mike Wilkins, the Willowbrook doctor who helped organize parents to shut down the institution in 1987, also doesn’t think that the experiments are black-and-white. “I’m not wanting to crucify Krugman,” he says now, “hepatitis B, for God sakes, is an international disease that there’s now a vaccine for. But let’s never ever do that again.”
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Sanofi-Aventis agreed to pay $109 million to resolve allegations that the company gave doctors free units of Hyalgan (an injection to relieve knee pain) to encourage those doctors to buy their product. Sanofi lowered the effective price by promising these free samples to doctors, but at the same time got inflated prices from government programs by submitting false price reports, alleged the United States. Medicare and other government health care programs “paid millions of dollars in kickback-tainted claims for Hyalgan,” according to the DOJ announcement.
9
Endo
FEB 2014
Endo Health Solutions Inc. and its subsidiary Endo Pharmaceuticals Inc. agreed to pay $192.7 million to resolve criminal and civil liability arising from Endo’s marketing of the prescription drug Lidoderm. As part of the agreement, Endo admitted that it intended that Lidoderm be used for unapproved indications and that it promoted Lidoderm to healthcare providers this way.
8
AstraZeneca
APRIL 2010
AstraZeneca was fined $520 million to resolve allegations that it illegally promoted the antipsychotic drug Seroquel. The drug was approved for treating schizophrenia and later for bipolar mania, but the government alleged that AstraZeneca promoted Seroquel for a variety of unapproved uses, such as aggression, sleeplessness, anxiety, and depression. AstraZeneca denied the charges but agreed to pay the fine to end the investigation.
7
Amgen
DEC 2012
Amgen agreed to pay a $762 million fine to resolve criminal and civil charges that the company illegally introduced and promoted several drugs including Aranesp, a drug to treat anemia. Amgen pleaded guilty to illegally selling Aranesp to be used at doses that the FDA had explicitly rejected, and for an off-label treatment that had never been FDA-approved.
6
Merck
NOV 2011
Merck agreed to pay a fine of $950 million related to the illegal promotion of the painkiller Vioxx, which was withdrawn from the market in 2004 after studies found the drug increased the risk of heart attacks. The company pled guilty to having promoted Vioxx as a treatment for rheumatoid arthritis before it had been approved for that use. The settlement also resolved allegations that Merck made false or misleading statements about the drug’s heart safety to increase sales.
5
Eli Lilly
JAN 2009
Eli Lilly was fined $1.42 billion to resolve a government investigation into the off-label promotion of the antipsychotic Zyprexa. Zyprexa had been approved for the treatment of certain psychotic disorders, but Lilly admitted to promoting the drug in elderly populations to treat dementia. The government also alleged that Lilly targeted primary care physicians to promote Zyprexa for unapproved uses and “trained its sales force to disregard the law.”
4
Abbott
MAY 2012
Abbott was fined $1.5 billion in connection to the illegal promotion of the antipsychotic drug Depakote. Abbott admitted to having trained a special sales force to target nursing homes, marketing the drug for the control of aggression and agitation in elderly dementia patients. Depakote had never been approved for that purpose, and Abbott lacked evidence that the drug was safe or effective for those uses. The company also admitted to marketing Depakote to treat schizophrenia, even though no study had found it effective for that purpose.
3
Johnson & Johnson
NOV 2013
Johnson & Johnson agreed to pay a $2.2 billion fine to resolve criminal and civil allegations relating to the prescription drugs Risperdal, Invega and Natrecor. The government alleged that J&J promoted these drugs for uses not approved as safe and effective by the FDA, targeted elderly dementia patients in nursing homes, and paid kickbacks to physicians and to the nation’s largest long-term care pharmacy provider, Omnicare Inc. As part of the agreement, Johnson & Johnson admitted that it promoted Risperdal for treatment of psychotic symptoms in non-schizophrenic patients, although the drug was approved only to treat schizophrenia.
2
Pfizer
SEPT 2009
Pfizer was fined $2.3 billion, then the largest health care fraud settlement and the largest criminal fine ever imposed in the United States. Pfizer pled guilty to misbranding the painkiller Bextra with “the intent to defraud or mislead”, promoting the drug to treat acute pain at dosages the FDA had previously deemed dangerously high. Bextra was pulled from the market in 2005 due to safety concerns. The government alleged that Pfizer also promoted three other drugs illegally: the antipsychotic Geodon, an antibiotic Zyvox, and the antiepileptic drug Lyrica.
GlaxoSmithKline agreed to pay a fine of $3 billion to resolve civil and criminal liabilities regarding its promotion of drugs, as well as its failure to report safety data. This is the largest health care fraud settlement in the United States to date. The company pled guilty to misbranding the drug Paxil for treating depression in patients under 18, even though the drug had never been approved for that age group. GlaxoSmithKline also pled guilty to failing to disclose safety information about the diabetes drug Avandia to the FDA.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Sometimes my memes are 3D. And you can own them. Or send them to someone. You can even eat some of them. CLICK HERE
No, I’m not going tabloid, bare this knuckle-head with me for a minute!
I’m guilty of fermenting well-founded indignation against some celebritard and professional tough guy who last year was begging “the powers that be” (exact quote) to save his tough ass from the Macarenavirus by locking his people down and ruining their lives, with military intervention, if needed. You may have heard of this clown that goes around unsupervised, yet heavily guarded, under the name of Conor McGregor. He beats people for money and he’s very good at it, apparently, and that’s the least annoying thing about him. And thing is he has just addressed his stupidity, proving he has taken his vitamins and has grown half a testicle since. So I have the professional obligation (no, I don’t, but it’s a good lesson) to reflect his latest brain-fart accurately. Point being: if we don’t take our daily dose of intellectual vitamins, we end up like this nitwit. I sweat hard to make it easier, I provide, free of charge, donations welcome, and my monthly earnings from this probably can’t pay a ticked to this door-knob’s 5-minute performances. But l retain immensely more human dignity and tight sleep from my position. I wish you what you wish yourself after watching this:
This was early 2020 when people where “collapsing in the streets” I was scared for my family. I urged everyone to sit tight for a few weeks to see where we land. My opinion on this situation now is night and day to then. I actually feel I was lied to originally. As where we all.
No, dipshit, we weren’t all lied! As a matter of fact, many of us sounded the alarm long before you vomited that abomination, and you social parasites slandered us, some still do. You learned your lesson 20 years too late to be an useful member of your society. See about catching up before your tiny brain falls out through your big mouth! There’s no scientific evidence for a novel coronavirus, it all points at your novel species of remote-controlled brainless NPCs being the cause for the current societal collapse.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
This quote should be on her tombstone. That’s why I decided to help make it more popular.
Five years ago, Wellesley College released some audio excerpts of a 21-year-old Hillary Rodham Clinton speaking at her 1969 commencement. But no seems to have picked up on this part. The class selected Clinton as Wellesley’s first-ever student commencement speaker. Clinton discussed leadership, the political climate in the 1960s and making the art of the impossible, possible. Whatever that meant. You can learn more about Clinton’s years as a student by visiting http://www.wellesley.edu.
Seeing her following career achievements and her adoration speeches for people like Margaret Sanger, I’d say she kept the course and this was a more honest moment of her life.
Some people just don’t feel people feelings.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
We gave up on our profit shares from masks, if you want to help us, please use the donation button! We think frequent mask use, even short term use can be bad for you, but if you have no way around them, at least send a message of consciousness. Get it here!
Much like the Fed, CDC isn’t a government agency, it’s more like a prototype of today’s PPP’s (Private-Public Partnerships) used by the WEF to siphon public wealth into private pockets and subvert the political self-determination of the people.
One way for CDC to attract funds is their Foundation. And we can’t follow the money if we don’t even know who the sponsors are. If you had difficulties before in finding them, though I can’t imagine one, now you have no excuse, you just need to CLICK HERE to find out more about the conflict of interests in which Pharmafia thrives like a baby in the amniotic juice. Removing that womb would terminate this vile genocidal cartel. There’s more than just that page, but that’s where you start YOUR OWN RESEARCH.
Interestingly, the CDC Foundation self-portrait looks very much like Klaus Schwab:
“The CDC Foundation is an independent nonprofit and the sole entity created by Congress to mobilize philanthropic and private-sector resources to support the Centers for Disease Control and Prevention’s critical health protection work.
We are a catalyst for unleashing the power of collaboration between CDC and philanthropies, private entities and individuals to protect the health, safety and security of America and the world.
The government has unique capacities as well as limitations. The same is true for the private and philanthropic sectors. We believe that people, groups and organizations have greater positive impact and can accomplish more collectively than individually. By aligning diverse interests and resources and leveraging all parties’ strengths, our focused collaborations with private and philanthropic partners help create greater impact than any one entity can alone. Your support saves and improves lives—right now and in the future.
Thanks to our donors, we have launched approximately more than 1,200 health protection programs and raised over $1.2 billion to support CDC’s work over the past two decades. To keep people healthy, safe and secure, we managed hundreds of programs in the United States and in more than 140 countries.” – SOURCE
Now, to make my point, I just need to highlight some of the names found there, for your later references. These are some of the people who home-detain, muzzle and inject us. Interestingly, most of them are also partners in the World Economic Forum.
Before fusing humans with technology, the Schwaborg has fused Pharmafia with Big Tech, mainstream media and the Governments. These are not independent voices confirming one another, they’re the same entity, like the Borg (and I’ll prove later that Star Trek’s Borg is not just science-fiction entertainment).
If your nutritionist has a McDonalds badge, you have no nutritionist. Btw, many US and UK hospitals, maybe in other countries too, host McDonalds restaurants. Same people.
Some things are not meant to be businesses, public health is one of them.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
They knew about everything else, years ahead sometimes, so of course they’ve been aware of the jabs side-effects too… By means of hiding these from us, they actively infringed upon our right to informed consent, as per the Nuremberg Code.
FDA Safety Surveillance of COVID-19 Vaccines : DRAFT Working list of possible adverse event outcomes Subject to change
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
The latest piece of evidence to confirm many of the revelations we’ve published for the past year or so. You have to read back to get more of the picture we’re about to sketch here.
We can’t offer informed consent for these experiments conducted on us because we are not offered much information. Only rich people can access some of it at prices most of us can’t dream. Maybe you can, or maybe people start donating enough so we can afford surviving another month and buying this info for the purpose of making it freely available to everyone, as it should be.
What am I talking about is the book pictured in our cover illustration and detailed below, which costs well over 1000$!
More precisely $1185 just for a single license PDF, the hardcover print would cost you about 100 more.
Why is this thing so expensive, you may ask?
THESE INFORMATIONS ARE SO EXPENSIVE EXACTLY TO BE PROHIBITIVE TO THE PLEBS AND OFFER A LEVERAGE OVER THOSE WHO ARE KEPT OUT OF THE LOOP, IN THE DARK
Predictably so, but:
These informations also must to have the highest degree of accuracy in order to sell as expensively!
Superb quality book delivered in a timely fashion with full financial documentation received via email.
Testimonial by Dr Tom Kidd, Associate Professor, University of Nevada
Bonus for us, this book is from May 2020, so it must have been elaborated prior to April 2020. This means it might be outdated by now for investors, but witty investigators like us find an advantage in this:
THE BOOK HAS BEEN ELABORATED WITH BEHIND THE SCENES SCIENCE ON THE INDUSTRIES WHICH, IN TURN MUST HAVE HAD PRE-SCIENCE ON THE PLANDEMIC! There was no publicly available information in March to build such a book, and the industries they talk about must have been prescient, way ahead of the writers. Only the fact that this book existed in May 2020 is single-handedly proving there was a whole lot of awareness in some industries about the pandemic. Corroborated with all other evidence we’ve provided on this website, pandemic pre-planning, ergo pre-science, becomes a certitude.
Until plebs learn the GameStop lesson properly and start associating their financial power to break this classism and this information gatekeeping, we have to be happy with whatever meat we can chew from the bones they throw out. Luckily for you, I can show you how to suck a bone dry and use it to find more. It’s not going to be a full course, but it might become more than most people can load up.
Let’s start with the description (highlights are mine):
“Nanotechnology and nanomaterials can significantly address the many clinical and public healthcare challenges that have arisen from the coronavirus pandemic. This analysis examines in detail how nanotechnology and nanomaterials can help in the fight against this pandemic disease, and ongoing mitigation strategies. Nano-based products are currently being developed and deployed for the containment, diagnosis, and treatment of Covid-19.
Nanotechnology and nanomaterials promise:
Improved and virus disabling air filtration.
Low-cost, scalable detection methods for the detection of viral particles
Enhanced personal protection equipment (PPE) including facemasks.
New antiviral vaccine and drug delivery platforms.
New therapeutic solutions.
Report contents include:
Market analysis of nano-based diagnostic tests for COVID-19 including nanosensors incorporating gold nanoparticles, iron oxide nanoparticles, graphene, quantum dots, carbon quantum dots and carbon nanotubes. Market revenues adjusted to pandemic outcomes. In-depth company profiles. Companies profiled include Abbott Laboratories, Cardea, Ferrotec (USA) Corporation, E25Bio, Grolltex, Inc., Luminex Corporation etc.
Market analysis of antiviral and antimicrobial nanocoatings for surfaces including fabric (mask, gloves, doctor coats, curtains, bed sheet), metal (lifts, doors handle, nobs, railings, public transport), wood (furniture, floors and partition panels), concrete (hospitals, clinics and isolation wards) and plastics (switches, kitchen and home appliances).
Market revenues adjusted to pandemic outcomes. In-depth company profiles. Companies profiled include Advanced Materials-JTJ s.r.o., Bio-Fence, Bio-Gate AG, Covalon Technologies Ltd., EnvisionSQ, GrapheneCA, Integricote, Nano Came Co. Ltd., NanoTouch Materials, LLC, NitroPep and many more.
Market analysis of air-borne virus filtration including photocatalytic Nano-TiO2 filters, nanofiber filers, nanosilver, nanocellulose, graphene and carbon nanotube filtration. Market revenues adjusted to pandemic outcomes. In-depth company profiles. Companies profiled include G6 Materials, Daicel FineChem Ltd., NANOVIA s.r.o., Toray Industries, Inc., Tortech Nano Fibers etc.
Market analysis of nano-based facemask and other PPE products. Market revenues adjusted to pandemic outcomes. In-depth company profiles. Companies profiled include planarTECH LLC, RESPILON Group s. r. o., SITA, Sonovia Ltd. etc.
Nanotherapies and drug delivery vehicles currently being produced and clinical trials of vaccines for COVID-19. Market revenues adjusted to pandemic outcomes. In-depth company profiles. In-depth company profiles. Companies profiled include Arcturus Therapeutics, Inc., Arbutus Biopharma, BlueWillow Biologics, Elastrin Therapeutics Inc., EnGeneIC Ltd. etc.
Key scientific breakthroughs and developments that are underway right now.”
As you can see, the description alone offers enough evidence that embedding a whole range of nanotech in facemasks, tests, drugs and many other product.
You can bet your ass your new fridge connect to the internet and has some antimicrobial nanocoating that later will prove to be worse than DDT or asbestos, but at least it’s not gonna be Covid, right?
“You could put the computational power of the spaceship Voyager onto an object the size of a cell”. And that was back in 2018
Can we dig more clues though?
Sir, yes, sir!
I’m going to do something unusual and seemingly unpractical copying here the whole table of contents, just in case, because almost every chapter and figure title deserves to be a separate post on this website as well, besides the multitude of leads as to what to research.
1 RESEARCH SCOPE AND METHODOLOGY 1.1 Report scope 1.2 Research methodology
2 INTRODUCTION
3 DIAGNOSTIC TESTING 3.1 Nanotechnology and nanomaterials solutions 3.1.1 Current Diagnostic Tests for COVID-19 3.1.2 Emerging Diagnostic Tests for COVID-19 3.1.3 Nanosensors/nanoparticles (silver nanoclusters, Gold nanoparticles, Iron oxide nanoparticles, Quantum dot barcoding, nanowires, silica nanoparticles) 3.1.4 Carbon nanomaterials for diagnostic testing 3.2 Market revenues 3.2.1 Market estimates adjusted to pandemic demand, forecast to 2025. 3.3 Companies 3.4 Academic research
4 ANTIVIRAL AND ANTIMICROBIAL COATINGS AND SURFACES 4.1 Nanotechnology and nanomaterials solutions 4.1.1 Nanocoatings. 4.1.2 Applications 4.1.3 Anti-viral nanoparticles and nanocoatings 4.1.3.1 Reusable Personal Protective Equipment (PPE) 4.1.3.2 Wipe on coatings 4.1.4 Graphene-based coatings 4.1.4.1 Properties 4.1.4.2 Graphene oxide. 4.1.4.3 Reduced graphene oxide (rGO) 4.1.4.4 Markets and applications 4.1.5 Silicon dioxide/silica nanoparticles (Nano-SiO2) -based coatings 4.1.5.1 Properties. 4.1.5.2 Antimicrobial and antiviral activity 4.1.5.3 Easy-clean and dirt repellent 4.1.6 Nanosilver-based coatings. 4.1.6.1 Properties 4.1.6.2 Antimicrobial and antiviral activity 4.1.6.3 Markets and applications. 4.1.6.4 Commercial activity 4.1.7 Titanium dioxide nanoparticle-based coatings 4.1.7.1 Properties 4.1.7.2 Exterior and construction glass coatings 4.1.7.3 Outdoor air pollution 4.1.7.4 Interior coatings 4.1.7.5 Medical facilities 4.1.7.6 Wastewater Treatment 4.1.7.7 Antimicrobial coating indoor light activation 4.1.8 Zinc oxide nanoparticle-based coatings 4.1.8.1 Properties. 4.1.8.2 Antimicrobial activity 4.1.9 Nanocellullose (cellulose nanofibers and cellulose nanocrystals)-based coatings. 4.1.9.1 Properties 4.1.9.2 Antimicrobial activity 4.1.10 Carbon nanotube-based coatings 4.1.10.1 Properties 4.1.10.2 Antimicrobial activity 4.1.11 Fullerene-based coatings 4.1.11.1 Properties 4.1.11.2 Antimicrobial activity 4.1.12 Chitosan nanoparticle-based coatings 4.1.12.1 Properties 4.1.12.2 Wound dressings 4.1.12.3 Packaging coatings and films 4.1.12.4 Food storage 4.1.13 Copper nanoparticle-based coatings 4.1.13.1 Properties 4.1.13.2 Application in antimicrobial nanocoatings 4.2 Market revenues 4.2.1 Market revenues adjusted to pandemic demand, forecast to 2030. 4.3 Companies 4.4 Academic research
5 AIR-BORNE VIRUS FILTRATION 5.1 Nanotechnology and nanomaterials solutions (nanoparticles titanium dioxide, Polymeric nanofibers, Nanosilver, Nanocellulose, Graphene, Carbon nanotubes) 5.2 Market revenues 5.2.1 Market estimates adjusted to pandemic demand, forecast to 2025 5.3 Companies 5.4 Academic research
6 FACEMASKS AND OTHER PPE 6.1 Nanotechnology and nanomaterials solutions (Polymer nanofibers, Nanocellulose, Nanosilver, Graphene) 6.2 Market revenues 6.2.1 Market estimates adjusted to pandemic demand, forecast to 2025 6.3 Companies 6.4 Academic research
7 DRUG DELIVERY AND THERAPEUTICS 7.1 Nanotechnology and nanomaterials solutions 7.1.1 Products 7.1.2 Nanocarriers 7.1.3 Nanovaccines 7.2 Market revenues 7.2.1 Market estimates adjusted to pandemic demand, forecast to 2025 7.3 Companies 7.4 Academic research
8 REFERENCES
List of Tables Table 1. Current Diagnostic Tests for COVID-19 Table 2. Development phases of diagnostic tests Table 3. Emerging Diagnostic Tests for COVID-19 Table 4. Nanoparticles for diagnostic testing-Types of nanoparticles, properties and application Table 5. Gold nanoparticle reagent suppliers list Table 6. Carbon nanomaterials for diagnostic testing-types, properties and applications Table 7. Global revenues for nanotech-based diagnostics and testing, 2019-2030, millions US$, adjusted for COVID-19 related demand, conservative and high estimates Table 8. Academic research in nano-based COVID-19 diagnostics and testing. Table 9: Anti-microbial and antiviral nanocoatings-Nanomaterials used, principles, properties and applications. Table 10. Nanomaterials utilized in antimicrobial and antiviral nanocoatings coatings-benefits and applications. Table 11: Properties of nanocoatings. Table 12: Antimicrobial and antiviral nanocoatings markets and applications Table 13: Nanomaterials used in nanocoatings and applications. Table 14: Graphene properties relevant to application in coatings Table 15. Bactericidal characters of graphene-based materials Table 16. Markets and applications for antimicrobial and antiviral nanocoatings graphene nanocoatings Table 17. Markets and applications for antimicrobial and antiviral nanosilver coatings. Table 18. Commercial activity in antimicrobial nanosilver nanocoatings Table 19. Antibacterial effects of ZnO NPs in different bacterial species. Table 20. Types of carbon-based nanoparticles as antimicrobial agent, their mechanisms of action and characteristics Table 21. Mechanism of chitosan antimicrobial action Table 22. Global revenues for antimicrobial and antiviral nanocoatings, 2019-2030, US$, adjusted for COVID-19 related demand, conservative and high estimates. Table 23. Global revenues for Anti-fouling & easy clean nanocoatings, 2019-2030, US$, adjusted for COVID-19 related demand, conservative and high estimates. Table 24. Global revenues for self-cleaning (bionic) nanocoatings, 2019-2030, US$, adjusted for COVID-19 related demand, conservative and high estimates Table 25. Global revenues for self-cleaning (photocatalytic) nanocoatings, 2019-2030, US$, adjusted for COVID-19 related demand, conservative and high estimates Table 26. Antimicrobial, antiviral and antifungal nanocoatings research in academia Table 27. Cellulose nanofibers (CNF) membranes Table 28: Comparison of CNT membranes with other membrane technologies Table 29. Nanomaterials in air-borne virus filtration-properties and applications Table 30. Global revenues for nanotech-based air-borne virus filtration, 2019-2030, millions US$, adjusted for COVID-19 related demand, conservative and high estimates Table 31: Oji Holdings CNF products Table 32. Academic research in nano-based air-borne virus filtration Table 33. Nanomaterials in facemasks and other PPE-properties and applications Table 34. Global revenues for nanotech-based facemasks and PPE, 2019-2030, millions US$, adjusted for COVID-19 related demand, conservative and high estimates Table 35. Academic research in nano-based facemasks and other PPE Table 36. Applications in drug delivery and therapeutics, by nanomaterials type-properties and applications Table 37. Nanotechnology drug products Table 38. List of antigens delivered by using different nanocarriers Table 39. Nanoparticle-based vaccines Table 40. Global revenues for nano-based drug delivery and therapeutics, 2019-2030, billion US$, adjusted for COVID-19 related demand, conservative and high estimates Table 41. Academic research in nano-based drug delivery and therapeutics to address COVD-19
List of Figures Figure 1. Anatomy of COVID-19 Virus Figure 2. Graphene-based sensors for health monitoring Figure 3. Schematic of COVID-19 FET sensor incorporating graphene Figure 4. Global revenues for nanotech-based diagnostics and testing, 2019-2030, millions US$, adjusted for COVID-19 related demand, conservative and high estimates Figure 5. Printed graphene biosensors Figure 6. AGILE R100 system Figure 7. nano-screenMAG particles Figure 8. GFET sensors. Figure 9. DNA endonuclease-targeted CRISPR trans reporter (DETECTR) system Figure 10. SGTi-flex COVID-19 IgM/IgG Figure 11. Schematic of anti-viral coating using nano-actives for inactivation of any adhered virus on the surfaces Figure 12: Graphair membrane coating Figure 13: Antimicrobial activity of Graphene oxide (GO) Figure 14. Nano-coated self-cleaning touchscreen Figure 15: Hydrophobic easy-to-clean coating Figure 16 Anti-bacterial mechanism of silver nanoparticle coating. Figure 17: Mechanism of photocatalysis on a surface treated with TiO2 nanoparticles Figure 18: Schematic showing the self-cleaning phenomena on superhydrophilic surface. Figure 19: Titanium dioxide-coated glass (left) and ordinary glass (right). Figure 20: Self-Cleaning mechanism utilizing photooxidation. Figure 21: Schematic of photocatalytic air purifying pavement. Figure 22: Schematic of photocatalytic water purification Figure 23. Schematic of antibacterial activity of ZnO NPs Figure 24: Types of nanocellulose Figure 25. Mechanism of antimicrobial activity of carbon nanotubes Figure 26: Fullerene schematic Figure 27. TEM images of Burkholderia seminalis treated with (a, c) buffer (control) and (b, d) 2.0 mg/mL chitosan; (A: additional layer; B: membrane damage) Figure 28. Global revenues for antimicrobial and antiviral nanocoatings, 2019-2030, US$, adjusted for COVID-19 related demand, conservative and high estimates Figure 29. Global revenues for anti-fouling and easy-to-clean nanocoatings, 2019-2030, US$, adjusted for COVID-19 related demand, conservative and high estimates Figure 30. Global revenues for self-cleaning (bionic) nanocoatings, 2019-2030, US$, adjusted for COVID-19 related demand, conservative and high estimates Figure 31. Global revenues for self-cleaning (photocatalytic) nanocoatings, 2019-2030, US$, adjusted for COVID-19 related demand, conservative and high estimates Figure 32. Lab tests on DSP coatings Figure 33. GrapheneCA anti-bacterial and anti-viral coating Figure 34. Microlyte® Matrix bandage for surgical wounds Figure 35. Self-cleaning nanocoating applied to face masks. Figure 36. NanoSeptic surfaces. Figure 37. NascNanoTechnology personnel shown applying MEDICOAT to airport luggage carts Figure 38. Basic principle of photocatalyst TiO2 Figure 39. Schematic of photocatalytic indoor air purification filter. Figure 40. Global revenues for nanotech-based air-borne virus filtration, 2019-2030, millions US$, adjusted for COVID-19 related demand, conservative and high estimates. Figure 41. Multi-layered cross section of CNF-nw Figure 42: Properties of Asahi Kasei cellulose nanofiber nonwoven fabric Figure 43: CNF nonwoven fabric Figure 44: CNF gel.. Figure 45. CNF clear sheets Figure 46. Graphene anti-smog mask Figure 47. Global revenues for nanotech-based facemasks and PPE, 2019-2030, millions US$, adjusted for COVID-19 related demand, conservative and high estimates Figure 48. FNM’s nanofiber-based respiratory face mask.. Figure 49. ReSpimask® mask Figure 50. Schematic of different nanoparticles used for intranasal vaccination Figure 51. Global revenues for nano-based drug delivery and therapeutics, 2019-2030, billion US$, adjusted for COVID-19 related demand, conservative and high estimates.
So are you ready for your first “printed graphene bio-sensors”? Just picked a random item from the list above.
So what I’m going to do in the upcoming updates to this article is to follow every lead I got above, and I’m going to investigate every company they report on, as per their list below. You should do it too, independently, and compare your results with mine. It’s both science and investigative journalism, the juiciest combo.
Abbott Laboratories
Advanced Materials-JTJ s.r.o.
Arbutus Biopharma
Arcturus Therapeutics
Bio-Fence
Bio-Gate AG
BlueWillow Biologics
Cardea
Covalon Technologies Ltd.
Daicel FineChem Ltd.
E25Bio
Elastrin Therapeutics Inc.
EnGeneIC Ltd.
EnvisionSQ
Ferrotec (USA) Corporation
G6 Materials
GrapheneCA
Grolltex, Inc.
Integricote
Luminex Corporation
Nano Came Co. Ltd.
NanoTouch Materials, LLC
NANOVIA s.r.o.
NitroPep
RESPILON Group s. r. o.
SITA
Sonovia Ltd.
TECH LLC
Toray Industries
Tortech Nano Fibers
A taste of the future: Luminex, on of the companies listed above, makes PCR tests and stuff like magnetic micro-beads. They’ve just been bought for almost $2B by some Italians who can afford $1000+ books.
BESIDES THE DANGERS OF NANOBOTS, THIS INDUSTRY IS AN ENVIRONMENTAL CANCER AND A TOP CO2 PRODUCER
Ian Illuminato of Friends of the Earth says consumers deserve a say in nanotech regulation. JIM THOMAS/ETC GROUP
Nanotechnology was supposed to revolutionize the world, making us healthier and producing cleaner energy. But it’s starting to look more like a nightmare.
Nanomaterials—tiny particles as little as 1/100,000 the width of a human hair—have quietly been used since the 1990s in hundreds of everyday products, everything from food to baby bottles, pills, beer cans, computer keyboards, skin creams, shampoo, and clothes.
But after years of virtually unregulated use, scientists are now starting to say the most commonly used nanoproducts could be harming our health and the environment.
One of the most widespread nanoproducts is titanium dioxide. More than 5,000 tonnes of it are produced worldwide each year for use in food, toothpaste, cosmetics, paint, and paper (as a colouring agent), in medication and vitamin capsules (as a nonmedicinal filler), and in most sunscreens (for its anti-UV properties).
In food, titanium-dioxide nanoparticles are used as a whitener and brightener in confectionary products, cheeses, and sauces. Other nanoparticles are employed in flavourings and “nutritional” additives, and to reduce fat content in “health” foods.
In the journal Cancer Research in 2009, environmental-health professor Robert Schiestl coauthored the first comprehensive study of how titanium-dioxide nanoparticles affect the genes of live animals. Mice in his study suffered DNA and chromosomal damage after drinking water with the nanoparticles for five days.
“It should be removed from food and drugs, and there’s definitely no reason for it in cosmetic products,” said cancer specialist Schiestl, who is also a professor of pathology and radiation oncology at UCLA’s school of medicine.
“The study shows effects [from the nanoparticles] on all kinds of genetic endpoints,” Schiestl told the Georgia Straight in a phone interview from his office. “All those are precursor effects of cancer. It’s a wake-up call to do something.”
After Schiestl’s study came out, he said, he started getting calls from nervous people saying they had discovered titanium dioxide was listed as a nonmedicinal ingredient in their prescription medication. “They wanted to know how to get it out,” he said. “I said, ”˜I don’t know how to get it out.’ ”
Schiestl’s study is cited by groups like Greenpeace and Friends of the Earth in their calls for a moratorium on nanomaterials in food and consumer products.
“They were thought to be safe. Our study shows a lot of harm,” Schiestl said.
Nanoparticles can be harmful because they are so tiny they can pass deep into the skin, lungs, and blood. They are made by burning or crushing regular substances like titanium, silver, or iron until they turn into an ultrafine dust, which is used as a coating on, or ingredient in, various products.
Schiestl is now studying two other common nanoparticles, zinc oxide and cadmium oxide, and he has found they also cause DNA and chromosomal damage in mice.
Yet two years after Schiestl’s first study, titanium dioxide and other nanoparticles remain virtually unregulated in Canada and the U.S. Products containing nanoparticles still don’t have to be labelled, and manufacturers don’t have to prove they are safe for health or the environment.
In fact, only a small fraction of the hundreds of nanomaterials on the market have been studied to see if they are safe.
“The public has had little or no say on this. It’s mostly industry guiding government to make sure this material isn’t regulated,” said Ian Illuminato, a nanotech expert with Friends of the Earth, speaking from his home office in Victoria.
“Consumers aren’t given the right to avoid this. We think it’s dangerous and shouldn’t be in contact with the public and the environment,” he said.
Meanwhile, the number of products using nanomaterials worldwide has shot up sixfold in just a couple of years, from 212 in 2006 to more than 1,300 in 2011, according to a report in March by the Washington, D.C.–based Project on Emerging Nanotechnologies.
Those numbers are based on self-reporting by industry, and the real numbers are thought to be much higher. A Canadian government survey in 2009 found 1,600 nanoproducts available here, according to a report in December from the ETC Group, an Ottawa-based nonprofit that studies technology.
Nanotech is worth big money. More than $250 billion of nano-enabled products were produced globally in 2009, according to Lux Research, a Boston-based technology consultancy. That figure is expected to rise 10-fold, to $2.5 trillion, by 2015.
Lux Research estimated in 2006 that one-sixth of manufactured output would be based on nanotechnology by 2014.
Nanotech already appears to be affecting people’s health. In 2009, two Chinese factory workers died and another five were seriously injured in a plant that made paint containing nanoparticles.
The seven young female workers developed lung disease and rashes on their face and arms. Nanoparticles were found deep in the workers’ lungs.
“These cases arouse concern that long-term exposure to some nanoparticles without protective measures may be related to serious damage to human lungs,” wrote Chinese medical researchers in a 2009 study on the incident in the European Respiratory Journal.
When inhaled, some types of nanoparticles have been shown to act like asbestos, inflaming lung tissue and leading to cancer. In 2009, the World Health Organization’s International Agency for Cancer Research declared titanium dioxide to be “possibly carcinogenic to humans” after studies found that inhaling it in nanoparticle form caused rats to develop lung cancer and mice to suffer organ damage.
Nanoparticles can also hurt the skin. All those nanoparticles in skin creams and sunscreens may be behind a rise in eczema rates in the developed world, according to a 2009 study in the journal Experimental Biology and Medicine. The study found that titanium-dioxide nanoparticles caused mice to develop eczema. The nanoparticles “can play a significant role in the initiation and/or progression of skin diseases”, the study said.
Schiestl said nanoparticles could also be helping to fuel a rise in the rates of some cancers. He wouldn’t make a link with any specific kind of cancer, but data from the U.S. National Cancer Institute show that kidney and renal-pelvis cancer rates rose 24 percent between 2000 and 2007 in the U.S., while the rates for melanoma of the skin went up 29 percent and thyroid cancer rose 54 percent.
Schiestl said workers who deal with nanoparticles could be the most affected. That concern prompted the International Union of Food, Farm, and Hotel Workers to call in 2007 for a moratorium on commercial uses of nanotechnology in food and agriculture.
But despite all the health risks, we may already have run out of time to determine many of nanotech’s health impacts, Schiestl said.
“Nanomaterial is so ubiquitous that it would be very difficult to do an epidemiological study because there would be no control group of people who don’t use it.”
What happens when nanoparticles get out into the environment in wastewater or when products are thrown out?
Nanosilver is the most common nanomaterial on the market. Its extraordinary antimicrobial properties have earned it a place in a huge variety of products, including baby pacifiers, toothpaste, condoms, clothes, and cutting boards.
Virginia Walker, a biology professor at Queen’s University in Kingston, Ontario, decided to study nanosilver one day after a grad student said her mother had bought a new washing machine that doused clothes with silver nanoparticles to clean them better.
It sounded intriguing, Walker recalled thinking, but what would happen if nanosilver in the laundry water wound up in the environment? “What would it do to the bacterial communities out there?” she wondered.
On a whim, Walker decided to study the question. She figured the nanosilver would probably have no impact on beneficial microbes in the environment because any toxicity would be diluted.
“I did the experiment almost as a lark, not expecting to find anything,” she said by phone. “I hoped I would not find anything.”
In fact, Walker found that nanosilver was “highly toxic” to soil bacteria. It was especially toxic to one kind of nitrogen-fixing bacterium that is important to plant growth.
“If you had anything that was sensitive to nanoparticles, the last thing you would want is to have this microbe affected,” Walker said in a phone interview from her office.
The study prompted Walker to do more studies on nanoparticles. In one study now being reviewed for publication, one of her students found that mice exposed to nanoparticles developed skeletal abnormalities.
“People should have their eyes open. There are so many different nanoparticles, and the consequences of their use could be grave. We know almost nothing about these things,” Walker said.
Other scientists have raised concerns about nanosilver too. Some clothes makers now put it in socks and shirts, promising it will help control body odour. In a 2008 study in the Washington, D.C.–based journal Environmental Science and Technology, researchers took nanosilver-laced socks and washed them in water. They found the socks released up to half of their nanosilver into the water.
“If you start releasing ionic silver, it is detrimental to all aquatic biota. Once the silver ions get into the gills of fish, it’s a pretty efficient killer,” said study coauthor Troy Benn, a graduate student at Arizona State University, in a ScienceDaily.com story in 2008.
“I’ve spoken with a lot of people who don’t necessarily know what nanotechnology is, but they are out there buying products with nanoparticles in them.”
And what about the promise that nanotech could produce cleaner energy? The idea was that nanoparticles could make solar panels more efficient, be used as fuel additives to improve gas mileage, and make lighter cars and planes.
Most of the promised efficiency gains haven’t materialized, according to a 2010 report from Friends of the Earth. And it turns out that making nanomaterial is itself a huge energy guzzler.
A kilogram of carbon nanotubes—a nanoparticle used in cancer treatment and to strengthen sports equipment—requires an estimated 167 barrels of oil to produce, the Friends of the Earth report said.
Carbon nanotubes are “one of the most energy intensive materials known to humankind”, said a 2010 report to a symposium of the U.S.–based Institute of Electrical and Electronics Engineers.
That report said many nanoproducts may remain profitable despite their high energy cost only because of enormous government subsidies to the nanotech industry—$1.6 billion from the U.S. government last year.
But despite all this, regulation of nanotech remains glacially slow. The European Parliament voted nearly unanimously to recommend that nanoproducts be banned from food in 2009. But the European Commission rejected that recommendation last year, agreeing only that it may require labels on food containing nanomaterials. It will also require labels on cosmetics containing some nanoingredients starting in 2014.
Canada and the U.S. have yet to go even that far. At Health Canada, which regulates nanotechnology, a web page dealing with nanoproducts hasn’t been amended in four years and contains outdated information.
Health Canada spokesman Stéphane Shank did not return calls.
They used to say small is beautiful. But that was before small got scary. – Straight.com
NO MEANS NO, YES MEANS NO TOO
So yeah, that’s it for now, and if you think this is not enough to prove much, you can’t be more wrong, you’re probably bathing in dangerous or lethal nanotech as you read this, but feel free to return to this link in the coming days and weeks, I will be adding more evidence as I dig it out. I have about 100 leads there, it’s going to be a long process, friends!
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Take it with a pinch of salt, as per usual, this still a product of MIT.
Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19
Stephanie Seneff1 and Greg Nigh – Computer Science and Artificial Intelligence Laboratory, MIT, Cambridge MA, 02139, USA, E-mail: seneff@csail.mit.edu / Naturopathic Oncology, Immersion Health, Portland, OR 97214, USA
ABSTRACT
Operation Warp Speed brought to market in the United States two mRNA vaccines, produced by Pfizer and Moderna. Interim data suggested high efficacy for both of these vaccines, which helped legitimize Emergency Use Authorization (EUA) by the FDA.
However, the exceptionally rapid movement of these vaccines through controlled trials and into mass deployment raises multiple safety concerns. In this review we first describe the technology underlying these vaccines in detail.
We then review both components of and the intended biological response to these vaccines, including production of the spike protein itself, and their potential relationship to a wide range of both acute and long-term induced pathologies, such as blood disorders, neurodegenerative diseases and autoimmune diseases.
Among these potential induced pathologies, we discuss the relevance of prion-protein-related amino acid sequences within the spike protein. We also present a brief review of studies supporting the potential for spike protein “shedding”, transmission of the protein from a vaccinated to an unvaccinated person, resulting in symptoms induced in the latter.
We finish by addressing a common point of debate, namely, whether or not these vaccines could modify the DNA of those receiving the vaccination. While there are no studies demonstrating definitively that this is happening, we provide a plausible scenario, supported by previously established pathways for transformation and transport of genetic material, whereby injected mRNA could ultimately be incorporated into germ cell DNA for transgenerational transmission.
We conclude with our recommendations regarding surveillance that will help to clarify the long-term effects of these experimental drugs and allow us to better assess the true risk/benefit ratio of these novel technologies.
Introduction
Unprecedented. This word has defined so much about 2020 and the pandemic related to SARS-CoV-2. In addition to an unprecedented disease and its global response, COVID-19 also initiated an unprecedented process of vaccine research, production, testing, and public distribution (Shaw,
2021). The sense of urgency around combatting the virus led to the creation, in March 2020, of Operation Warp Speed (OWS), then-President Donald Trump’s program to bring a vaccine against COVID-19 to market as quickly as possible(Jacobs and Armstrong, 2020). OWS established a few more unprecedented aspects of COVID-19.
First, it brought the US Department of Defense into direct collaboration with US health departments with respect to vaccine distribution (Bonsell, 2021).
Second, the National Institutes of Health (NIH) collaborated with the biotechnology company Moderna in bringing an unprecedented type of vaccine against infectious disease to market, one utilizing a technology based on messenger RNA (mRNA) (National Institutes of Health, 2020).
The confluence of these unprecedented events has rapidly brought to public awareness the promise and potential of mRNA vaccines as a new weapon against infectious diseases into the future. At the same time, events without precedent are, by definition, without a history and context against which to fully assess risks, hoped-for benefits, safety, and long-term viability as a positive contribution to public health.
In this paper we will be briefly reviewing one particular aspect of these unprecedented events, namely the development and deployment of mRNA vaccines against the targeted class of infectious diseases under the umbrella of “SARS-CoV-2.
”We believe many of the issues we raise here will be applicable to any future mRNA vaccine that might be produced against other infectious agents, or in applications related to cancer and genetic diseases, while others seem specifically relevant to mRNA vaccines currently being implemented against the subclass of corona viruses. While the promises of this technology have been widely heralded, the objectively assessed risks and safety concerns have received far less detailed attention. It is our intention to review several highly concerning molecular aspects of infectious disease-related mRNA technology, and to correlate these with both documented and potential pathological effects.
UNPRECEDENTED
Many aspects of Covid-19 and subsequent vaccine development are unprecedented for a vaccine deployed for use in the general population.
Some of these includes the following.
First to use PEG (polyethylene glycol) in an injection (see text)
2. First to use mRNA vaccine technology against an infectious agent
3. First time Moderna has brought any product to market
4. First to have public health officials telling those receiving the vaccination to expect an adverse reaction
5. First to be implemented publicly with nothing more than preliminary efficacy data (see text)
6. First vaccine to make no clear claims about reducing infections, transmissibility, or deaths
7. First coronavirus vaccine ever attempted in humans
8. First injection of genetically modified polynucleotides in the general population
Vaccine Development
Development of mRNA vaccines against infectious disease is unprecedented in many ways. In a 2018 publication sponsored by the Bill and Melinda Gates Foundation, vaccines were divided into three categories: Simple, Complex, and Unprecedented (Young et al., 2018). Simple and Complex vaccines represented standard and modified applications of existing vaccine technologies.
Unprecedented represents a category of vaccine against a disease for which there has never before been a suitable vaccine. Vaccines against HIV and malaria are examples. As their analysis indicates, depicted in Figure 1, unprecedented vaccines are expected to take 12.5 years to develop. Even more ominously, they have a 5% estimated chance of making it through Phase II trials (assessing efficacy) and, of that 5%, a 40% chance of making it through Phase III trials (assessing population benefit). In other words, an unprecedented vaccine was predicted to have a 2% probability of success at the stage of a Phase III clinical trial. As the authors bluntly put it, there is a “low probability of success, especially for unprecedented vaccines.” (Young et al., 2018)
Figure 1.Launching innovative vaccines is costly and time-consuming, with a low probability of success, especially for unprecedented vaccines (adapted from Young et al, 2018).
With that in mind, two years later we have an unprecedented vaccine with reports of 90-95% efficacy (Baden et al. 2020). In fact, these reports of efficacy are the primary motivation behind public support of vaccination adoption (U.S. Department of Health and Human Services, 2020). This defies not only predictions, but also expectations.
The British Medical Journal(BMJ) may be the only prominent conventional medical publication that has given a platform to voices calling attention to concerns around the efficacy of the COVID-19 vaccines. There are indeed reasons to believe that estimations of efficacy are in need of re-evaluation. Peter Doshi, an associate editor of the BMJ, has published two important analyses (Doshi 2021a, 2021b) of the raw data released to the FDA by the vaccine makers, data that are the basis for the claim of high efficacy. Unfortunately, these were published to the BMJ’s blog and not in its peer-reviewed content. Doshi, though, has published a study regarding vaccine efficacy and the questionable utility of vaccine trial endpoints in BMJ’s peer reviewed content (Doshi 2020).
A central aspect of Doshi’s critique of the preliminary efficacy data is the exclusion of over 3400 “suspected COVID-19 cases” that were not included in the interim analysis of the Pfizer vaccine data submitted to the FDA. Further, a low-but-non-trivial percent of individuals in both Moderna and Pfizer trials were deemed to be SARS-CoV-1-positive at baseline despite prior infection being grounds for exclusion. For these and other reasons the interim efficacy estimate of around 95% for both vaccines is suspect.
A more recent analysis looked specifically at the issue of relative vs. absolute risk reduction. While the high estimates of risk reduction are based upon relative risks, the absolute risk reduction is a more appropriate metric for a member of the general public to determine whether a vaccination provides a meaningful risk reduction personally. In that analysis, utilizing data supplied by the vaccine makers to the FDA, the Moderna vaccine at the time of interim analysis demonstrated an absolute risk reduction of 1.1% (p= 0.004), while the Pfizer vaccine absolute risk reduction was 0.7% (p<0.000) (Brown 2021).
Others have brought up important additional questions regarding COVID-19 vaccine development, questions with direct relevance to the mRNA vaccines reviewed here.
For example, Haidere, et. al. (2021) identify four “critical questions” related to development of these vaccines, questions that are germane to both their safety and their efficacy:
•Will Vaccines Stimulate the Immune Response?
•Will Vaccines Provide Sustainable Immune Endurance?
•How Will SARS-CoV-2 Mutate?
•Are We Prepared for Vaccine Backfires?
Lack of standard and extended preclinical and clinical trials of the two implemented mRNA vaccines leaves each of these questions to be answered over time. It is now only through observation of pertinent physiological and epidemiological data generated by widescale delivery of the vaccines to the general public that these questions will be resolved. And this is only possible if there is free access to unbiased reporting of outcomes –something that seems unlikely given the widespread censorship of vaccine-related information because of the perceived need to declare success at all cost.
The two mRNA vaccines that have made it through phase 3 trials and are now being delivered to the general population are the Moderna vaccine and the Pfizer-BioNTech vaccine.
The vaccines have much in common. Both are based on mRNA encoding the spike protein of the SARS-CoV-2 virus. Both demonstrated a relative efficacy rate of 94-95%. Preliminary indications are that antibodies are still present after three months. Both recommend two doses spaced by three or four weeks, and recently there are reports of annual booster injections being necessary (Mahose, 2021). Both are delivered through muscle injection, and both require deep-freeze storage to keep the RNA from breaking down. This is because, unlike double-stranded DNA which is very stable, single-strand RNA products are apt to be damaged or rendered powerless at warm temperatures and must be kept extremely cold to retain their potential efficacy (Pushparajah et al., 2021).
It is claimed by the manufacturers that the Pfizer vaccine requires storage at -94 degrees Fahrenheit (-70 degrees Celsius), which makes it very challenging to transport it and keep it cold during the interim before it is finally administered. The Moderna vaccine can be stored for 6 months at -4 degrees Fahrenheit (-20 degrees Celsius), and it can be stored safely in the refrigerator for 30 days following thawing (Zimmer et al., 2021).
Two other vaccines that are now being administered under emergency use are the Johnson & Johnson vaccine and the AstraZeneca vaccine. Both are based on a vector DNA technology that is very different from the technology used inthe mRNA vaccines.
While these vaccines were also rushed to market with insufficient evaluation, they are not the subject of this paper so we will just describe briefly how they are developed. These vaccines are based on a defective version of an adenovirus, a double-stranded DNA virus that causes the common cold.
The adenovirus has been genetically modified in two ways, such that it cannot replicate due to critical missing genes, and its genome has been augmented with the DNA code for the SARS-CoV-2 spike protein. AstraZeneca’s production involves an immortalized human cell line called Human Embryonic Kidney (HEK) 293, which is grown in culture along with the defective viruses (Dicks et al., 2012).
The HEK cell line was genetically modified back in the 1970s by augmenting its DNA with segments from an adenovirus that supply the missing genes needed for replication of the defective virus (Louis et al., 1997).
Johnson & Johnson uses a similar technique based on a fetal retinal cell line. Because the manufacture of these vaccines requires genetically modified human tumor cell lines, there is the potential for human DNA contamination as well as many other potential contaminants.
The media has generated a great deal of excitement about this revolutionary technology, but there are also concerns that we may not be realizing the complexity of the body’s potential for reactions to foreign mRNA and other ingredients in these vaccines that go far beyond the simple goal of tricking the body into producing antibodies to the spike protein.
In the remainder of this paper, we will first describe in more detail the technology behind mRNA vaccines. We devote several sections to specific aspects of the mRNA vaccines that concern us with regard to potential for both predictable and unpredictable negative consequences.
We conclude with a plea to governments and the pharmaceutical industry to consider exercising greater caution in the current undertaking to vaccinate as many people as possible against SARS-CoV-2.
Experimental mRNA vaccines have been heralded as having the potential for great benefits, but they also harbor the possibility of potentially tragic and even catastrophic unforeseen consequences.
The mRNA vaccines against SARS-CoV-2 have been implemented with great fanfare, but there are many aspects of their widespread utilization that merit concern. We have reviewed some, but not all, of those concerns here, and we want to emphasize that these concerns are potentially serious and might not be evident for years or even transgenerationally.
In order to adequately rule out the adverse potentialities described in this paper, we recommend, at a minimum, that the following research and surveillance practices be adopted:
•A national effort to collect detailed data on adverse events associated with the mRNA vaccines with abundant funding allocation, tracked well beyond the first couple of weeks after vaccination.
•Repeated autoantibody testing of the vaccine-recipient population. The autoantibodies tested could be standardized and should be based upon previously documented antibodies and autoantibodies potentially elicited by the spike protein. These include autoantibodies against phospholipids, collagen, actin, thyroperoxidase (TPO), myelin basic protein, tissue transglutaminase, and perhaps others.
•Immunological profiling related to cytokine balance and related biological effects. Tests should include, at a minimum, IL-6, INF-α, D-dimer, fibrinogen, and C-reactive protein.
•Studies comparing populations who were vaccinated with the mRNA vaccines and those who were not to confirm the expected decreased infection rate and milder symptoms of the vaccinated group, while at the same time comparing the rates of various autoimmune diseases and prion diseases in the same two populations.
•Studies to assess whether it is possible for an unvaccinated person to acquire vaccine-specific forms of the spike proteins from a vaccinated person in close proximity.
•In vitro studies to assess whether the mRNA nanoparticles can be taken up by sperm and converted into cDNA plasmids.
•Animal studies to determine whether vaccination shortly before conception can result in offspring carrying spike-protein-encoding plasmids in their tissues, possibly integrated into their genome.
•In vitro studies aimed to better understand the toxicity of the spike protein to the brain, heart, testes, etc.
Public policy around mass vaccination has generally proceeded on the assumption that the risk/benefit ratio for the novel mRNA vaccines is a “slam dunk.” With the massive vaccination campaign well under way in response to the declared international emergency of COVID-19, we have rushed into vaccine experiments on a world-wide scale. At the very least, we should take advantage of the data that are available from these experiments to learn more about this new and previously untested technology. And, in the future, we urge governments to proceed with more caution in the face of new biotechnologies.
Finally, as an obvious but tragically ignored suggestion, the government should also be encouraging the population to take safe and affordable steps to boost their immune systems naturally, such as getting out in the sunlight to raise vitamin D levels (Ali, 2020), and eating mainly organic whole foods rather than chemical-laden processed foods (Rico-Campà et al., 2019). Also, eating foods that are good sources of vitamin A, vitamin C and vitamin K2 should be encouraged, as deficiencies in these vitamins are linked to bad outcomes from COVID-19 (Goddek, 2020; Sarohan, 2020).
Acknowledgements
This research was funded in part by Quanta Computers, Inc., Taiwan, under the auspices of the Qmulus project.Competing interests
The authors have no competing interests or conflicts to declare.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
The rare media reports on this case only mention WHO’s chief scientist, but after obtaining the original legal notice from IBA, we find out that Tedros and one more doctor are equally indicted. The best part is that they repeatedly use the term “conspiracy”, and, finally, someone uses it correctly.
Quick update as of July 14th, 2021: I’ve just learned of two more similar court cases that also involve Bill Gates, Fauci and GAVI, among others. Currently analyzing the documents and digging for more info. I will report more ASAP.
LEGAL NOTICE FOR CONTEMPT OF COURT AGAINST DR. TEDROS ADHANOM GHEBREYESUS, DR. SOUMYA SWAMINATHAN AND THE DIRECTORATE GENERAL OF HEALTH SERVICES (DGHS)
LEGAL NOTICE FOR CONTEMPT OF COURT AGAINST DR. TEDROS ADHANOM GHEBREYESUS, DR. SOUMYA SWAMINATHAN AND THE DIRECTORATE GENERAL OF HEALTH SERVICES (DGHS)
The accused are served legal notice for their attempt to undermine the authority of the Bombay High Court and obstruct the use of Ivermectin for Covid-19 treatment.
On 13th June 2021, Indian Bar Association has served a notice upon Dr.Tedros Adhanom Ghebreyesus, Director General, World Health Organisation, Dr.Soumya Swaminathan, the Chief Scientist at WHO and Prof. (Dr.) Sunil Kumar for contempt of judgment of Bombay High Court.
The Bombay High Court vide its judgment dated 28th May 2021 has already given a green signal for use of Ivermectin for treatment of Covid-19.
Despite this, all the three contemnors have hatched a conspiracy and by spreading misinformation through media, are fuelling confusion amongst doctors by introducing Guidelines allegedly published on 27th May 2021 by DGHS, which are in fact not mandatory and are overruled by the judgment of Bombay High Court dated 28thMay 2021.
The State Government of Goa, in their affidavit filed before Bombay High Court, has specifically pointed out that the WHO advisory against the use of Ivermectin is flawed and the research showed that the Ivermectin is effective for treatment of COVID-19. The Bombay High Court on 28th May 2021, after considering WHO advisory and all other contentions of the rival parties, came to the conclusion that the use of Ivermectin cannot be stopped. The High Court has also taken the note of the guidelines dated 17th May 2021 issued by Indian Council of Medical Research (ICMR), thereby advocating the use of Ivermectin.
Thereafter, a detailed and impactful article was published by the leading newspaper ‘Free Press Journal’ on 6th June 2021 (updated on 14th June 2021) wherein the author has articulated very well as to how the advisories of WHO are dubious.
Surprisingly, in its first, the Directorate of Health Services (DGHA) on 27th May, 2021 announced ‘Comprehensive Guidelines for Management of COVID-19 patients’ which excludes Ivermectin and several popular drugs.
It is worthwhile to note that DGHS is a repository of technical knowledge and is an attached organisation of the Ministry of Health & Family Welfare. The Guidelines/National Protocol have always been issued by the Joint Task Force of All India Institute of Medical Science (AIIMS) and Indian Council for Medical Research (ICMR) under the aegis of Government of India. Moreover, the document containing these impugned Guidelines does mention version/date and does not carry logos of Government of India, ICMR and AIIMS,suggesting lack of consensus between DGHS and the Joint Task Force.
Now, in order to diminish the impact of the article published on 6th June, 2021, the main accused Dr. Soumya Swaminathan hatched a conspiracy and managed some media houses to publish news on 7th June, 2021 for appreciating the overruled guidelines dated 27th May, 2021. Some of these media houses have showed astounding alacrity in publishing news hailing removal of Ivermectin and other drugs, thereby deliberately ignoring the mountains of clinical data on effectiveness of Ivermectin in treatment of COVID-19.
These impugned Guidelines issued by DGHS were circulated first on 7th June 2021, without any mention of the judgment of Bombay High Court dated 28thMay, 2021, which in fact is against the said guidelines, rendering these guidelines as null and void.
As per the judgment of Supreme Court of India, the person responsible for spreading information with object of creating confusion and to obstruct and undermine the judgment of court is liable for punishment under contempt of Court. Sections like 505,192,302, 115,109,409,120(B) of the Indian Penal Code are also attracted against the accused in this case, as their intention was to kill several people to fulfil their ulterior purposes.
The maximum punishment in above cases is death penalty.
The notice states that Dr. Soumya Swaminathan and the WHO are dishonest and have no scientific evidences to back their advisories and such loose statements are issued from time to time, to serve their ulterior purposes.
The relevant part of the notice reads this:
“53.1. Each time and particularly from following specific instances, it is sufficiently proved that You Notice 1 & 2 do not possess any authentic and scientific evidences;
i) When the earlier Notice was served on Notice 1 on 25.05.2021, she has neither replied to the notice nor has she approached any court of law against us. On the contrary, she chose to delete the controversial tweet advising against the use of Ivermectin for COVID-19;
ii) When the Health Secretary of the State Government of Goa relying on affidavit of Under Secretary of Union of India made their submission on oath before Hon’ble High Court, with specific allegations against WHO that there are reports which have observed that the analysis by WHO on this medicine (IVERMECTIN) is flawed and that the mortality rate is actually much lower if the said medicine is used for early treatment as well as prophylaxis, neither you Notice 1 or 2 chose to produce any proof to counter the said report. As a result, Hon’ble High Court has refused to accept the advisory of WHO.
iii) When All India Institute of Medical Science (AIIMS) had published a statement on 24.05.2021 that there is no evidence to predict the third wave and its effect on children, you Notice 1 did not give any “Evidence” in support of your statement dated 25.05.2021 which was contrary to the said statement of AIIMS.
After you Notice 1 were served with legal notice on 25.05.2021, you feared for being exposed and being summoned in Court of Law and therefore you Notice 1 took a U turn and stated that there is no sufficient evidence to suggest that children would be affected in the third wave.
The agenda of misinformation is also exposed in the statement published in Press Bureau of India on June 8, 2021
“It is a piece of misinformation that subsequent waves of the COVID-19 pandemic are going to cause severe illness in children. There is no data – either from India or globally – to show that children will be seriously infected in subsequent waves.”
53.2. So it is crystal clear that You Notice 1 & 2 do not have scientific evidence except jugglery of words and you are thoroughly intellectually dishonest people who are playing with the lives and livelihood of the common people across the world.
However, in order to expose your intellectual dishonesty to the entire world, this notice is being served, calling for an explanation within 7 days of the receipt of this notice.”
The legal notice also explains the law of damages in India citing recently cases where Court had ordered compensation of Rs. 100 Crores ((USD 13.5 mn) to the aggrieved party, for loss of his reputation. Since the present matter involves death caused due to denial of early treatment resulting in deterioration and death of person, the damages claimed would be much higher that Rs. 100 Crores.
The notice also explains the liability of Dr. Tedros Adhanom Ghebreyesus, Director General of WHO, for his act of commission and omission and also for his implied consent to the conspiracy.
In the similar manner, the DGHS Prof. (Dr.) Sunil Kumar is joined in as co-accused for his complicity in the conspiracy.
The three possible explanations for such an intense opposition to the use of highly promising, well-tolerated off-label medicine as Ivermectin are explained very well in following article:
“As a generic, Ivermectin is cheap and widely available, which means there would be a lot less money to be made by Big Pharma if it became the go-to early-stage treatment against covid.
Other pharmaceutical companies are developing their own novel treatments for Covid-19 which would have to compete directly with Ivermectin.
If approved as a covid-19 treatment, Ivermectin could even threaten the Emergency Use Authorisation granted to covid-19 vaccines.
It’s worth noting that while India’s DGHS has dumped most cheap off-patent treatment options against Covid, including even multivitamins, more expensive patented medicines continue to get the green light. They include Gilead’s prohibitively expensive antiviral Remdesivir, which DGHS continues to recommend for “select moderate/ severe hospitalised COVID-19 patients”, even though “it is only an experimental drug with potential to harm.” It has also authorised the use of the anti-inflammatory medicine to cilizumab, which costs hundreds of dollars a dose.” – IBA
I’m not very optimistic, I see this as another attempt to cement the existence of a fake virus in the collective mental, but either way this goes, the implications are huge. Consider that WHO didn’t act alone, Big Tech, mass-mediots and politicians would be affected by the same logic and principles. And if this falls flat, it’s only going to signal more corruption to the general population.
BUT, MOST IMPORTANTLY, IF THESE DRUGS ARE OFFICIALLY RECOGNIZED AS EFFICIENT AGAINST COVID-19, THEN THERE HAS NEVER BEEN A LEGAL BASIS FOR EMERGENCY STATES / EMERGENCY AUTHORIZATIONS FOR EXPERIMENTAL INJECTIONS DISGUISED AS VACCINES
If approved as a covid-19 treatment, Ivermectin could even threaten the Emergency Use Authorisation granted to covid-19 vaccines.
IBA
Demand from India to #ArrestDrTedros grows louder on social media
Dr Tedros Adhanom Ghebreyesus, Director-General, World Health Organisation
Panjim: The call from journalist and social activist Savio Rodrigues encouraging people of India to raise their voices on social media platform Twitter demanding arrest Dr Tedros Adhanom Ghebreyesus is growing louder.
#ArrestDrTedros is currently trending in India.
Savio Rodrigues is the Founder & Editor-in-Chief of GoaChronicle.com. The online new portal has been exposing the complicit role of Dr Tedros during the coronavirus pandemic due to his closeness with China. In fact, Rodrigues, opines that China backed Dr Tedros to the position of Director-General of the World Health Organisation (WHO) and Dr Tedros in turn was China’s puppet in WHO
Rodrigues in his several informative articles has raised questions on the dereliction of duty and cover-up of China’s questionable actions by the Director-General of (WHO).
Earlier today Rodrigues called for the people of India to unite and demand for the arrest of Dr Tedros, post the publishing of his article:
— Wg Cdr Nitin Purandare (Retd) 🇮🇳 (@nitinpurandare) April 11, 2020
Rodrigues opines : “The World Health Organisation under the leadership of its Director-General Dr Tedros Adhanom Ghebreyesus failed in its core responsibility to detect a health crisis and contain the spread of this contagious virus globally.
It instead chose to side with China – the nation from which the coronavirus originates and was the first epicentre of the virus. It is from Wuhan, China that the China Virus has spread globally to reportedly 180 countries.
We can go pontificating on different theories of the blame game. The political leaders can continue to play their own political games. Nothing will ever change the truth.
The truth is that this is a virus that has come out of a lab. The truth is that China had knowledge about its human-to-human transmission as early as December. The truth is that Dr Tedros relied on the report of the Chinese Health Authorities in his statement on January 14, 2020, “No clear evidence of human-to-human transmission. The truth is that China has withdrawn the lockdown in Wuhan and city is back to normal business will the rest of the world is under lockdown.
But the most horrific truth is people are dying. They will continue to die. We have crossed 100,000 deaths but the count will not cease, it will only keep on increasing.”
Whether Dr Tedros is arrested is a question that can only be in answered in time but what is important to state the noise to get him to step down from his post is certainly getting louder.
Tedros is met with treason and genocide accusations even in his own country, Ethiopia, but the government there simply doesn’t have the balls to anger Tedros’ allies issuing and arrest warrant to complete the investigation. However, the chief of Ethiopian military, as well as much of Indian media and population, don’t seem to hold back anymore. It’s doubtful he’s ever going to step home again.
After India finally gets somewhat of a grip on its deadly second wave, one of its health regulators just took away one of its main lines of defense.
India’s Directorate General of Health Services (DGHS) has executed a policy reversal that could have massive implications for the battle against covid-19, not only in India but around the world. Hundreds of thousands, if not millions of lives, could be at stake. The health regulator has overhauled its COVID-19 treatment guidelines and removed almost all of the repurposed medicines it had previously recommended for treating asymptomatic and mild cases. They include the antibiotic doxycycline, hydroxychloroquine, zinc, ivermectin and even multivitamins. The only medicines that are still recommended for early treatment are cold medicines, antipyretics such as paracetamol and inhaled budesonide.
“No other covid-specific medication [is] required,” say the new guidelines, which also discourage practitioners from prescribing unnecessary tests such as CT scans.
“Patients are advised to seek tele consultation; and Covid-19 appropriate behaviour must be observed such as mask, strict hand hygiene and physical distancing… [Patients are also advised to maintain] a healthy diet with proper hydration… [and] to stay connected [with family] and engage in positive talks through phone, video-calls, etc.”
The decision to remove ivermectin, multivitamins and zinc from the treatment guidelines is hard to comprehend given the current state of play in India — unless one assumes foul play. After suffering one of the worst covid-19 outbreaks since the pandemic began, resulting in the loss of hundreds of thousands of lives, India is not just flattening the curve, it is crushing it. And the widespread use of ivermectin, a potent anti-viral and anti-inflammatory with an excellent safety profile, appears to have played an instrumental role.
This is the last thing the World Health Organization (WHO) and the pharmaceutical companies whose interests it broadly represents want. As such, it was no surprise that WHO was delighted with the DGHS’ policy reversal. “Evidence based guidelines from @mohfw DGHS – simple, rational and clear guidance for physicians,” tweeted WHO’s chief scientist Soumya Swaminathan, of Indian descent. “Should be translated and disseminated in all Indian languages.”
As a generic, ivermectin is cheap and widely available, which means there would be a lot less money to be made by Big Pharma if it became the go-to early-stage treatment against covid.
Other pharmaceutical companies are developing their own novel treatments for Covid-19 which would have to compete directly with ivermectin.
If approved as a covid-19 treatment, ivermectin could even threaten the emergency use authorisation granted to covid-19 vaccines.
It’s worth noting that while India’s DGHS has dumped most cheap off-patent treatment options against Covid, including even multivitamins, more expensive patented medicines continue to get the green light. They include Gilead’s prohibitively expensive antiviral Remdesivir, which DGHS continues to recommend for “select moderate/ severe hospitalised COVID-19 patients”, even though “it is only an experimental drug with potential to harm.” It has also authorised the use of the anti-inflammatory medicine tocilizumab, which costs hundreds of dollars a dose.
Crushing the Curve
The DGHS began recommending the widespread use of ivermectin as early as April, in direct contradiction of the recommendations of the World Health Organization. Treatment packs were assembled in many states and distributed to patients testing positive for Covid. In at least two states — Goa and Uttarakhand — the medicine was distributed as a preventive. As has already happened in over 20 countries where ivermectin has been used — from Mexico, the Dominican Republic and Peru to Slovakia, the Czech Republic and Bangladesh — case numbers, hospitalizations and fatalities have fallen in almost vertical fashion. On Monday the country recorded its lowest number of new cases in 61 days.
“When we started seeing more cases, we decided to take up a door-to-door survey,” Bagalkot District Health Officer Dr Ananth Desai told New India Express. “When the health officials noticed people with symptoms during the survey, they tested them immediately and provided them with home isolation kits, which had medicines like Ivermectin, calcium and zinc tablets along with paracetamol. We advised the patients to start with the medication even before their Covid-19 test results came out. With these measures, we noticed that many patients recovered faster. This helped in increasing the recovery rate”.
In India’s capital, Delhi, the number of people testing positive for Covid-19 daily has fallen 97% from a peak of 24,000 on April 24. The number of deaths is down by around 85%. Only 17% of the total beds earmarked for Covid-19 treatment in Delhi and around 40% of the ICU beds were occupied late last week, according to the government’s Delhi Corona app. At the peak, there were days when no ICU beds were available in the city.
Out of the Darkness, But For How Long?
Just over four weeks ago India was in a very dark place. At one point it was accounting for almost half of all global cases and one in every four covid-19 deaths. The government had lost complete control. Four weeks later, the country, while not out of the woods, is in a much better place. While the official numbers of cases and deaths are probably still a fraction of the real numbers, the trend is clearly moving in the right direction.
An important reason for that is that doctors in India have been treating covid patients as early as possible — something that isn’t happening in most countries, particularly rich ones that play an outsized role in setting global health policy. In India early treatment has helped to reduce the number of cases becoming acute. And that has helped to reduce the pressure on hospitals and vital resources such as oxygen. Ivermectin also appears to have helped reduce the spread of the virus, thanks to its potent anti-viral properties.
Just about everywhere ivermectin is used, the number of cases, hospitalizations and deaths fall precipitously. Of course, this is only a temporal correlation. But nonetheless a clear pattern across nations and territories has formed that strongly supports ivermectin’s purported efficacy. And that efficacy has been amply demonstrated in dozens of clinical studies and multiple meta-analyses. But it’s not proof enough for global health authorities, which have set the bar for ivermectin so high that it’s almost impossible to straddle.
Of course, other factors such as lockdowns, travel restrictions and increased herd immunity have also played a part in India’s rapid turnaround. But vaccines’ role has been minimal given that just 16 doses have been administered per hundred people. It’s going to take many more months, if not longer, to vaccinate a majority of the population. In the meantime, hundreds of millions of people will remain unprotected from the virus. Many will end up catching and transmitting it. Yet the Directorate General of Health Services has taken away one of the country’s only lines of defense.
It remains to be seen whether state governors and health bureaucrats will comply with the recommendations. For the moment the separate treatment protocols recommended by India’s Ministry of Health and Family Welfare (MOHFW) and the Indian Council of Medical Research (ICMR) continue to include ivermectin. As such, many doctors are likely to continue prescribing the medicine. But what happens if MOHFW and ICMR follow the DGHS’ lead and also drop ivermectin. Will doctors stop using a medicine they know to work against a virus that has already caused so much devastation?
India’s most populous state, Uttar Pradesh, has been using ivermectin since last summer. In this second wave the turnaround was so dramatic that even the World Health Organization (WHO) showcased its achievements. In a May 7 article titled “Going the Last Mile to Stop Covid-19” the WHO noted that aggressive population-wide health schemes, including home testing and “medicine kits”, had helped regain control of the virus. But what the WHO failed to mention is what was in those medicine kits.
Instead, three days later WHO’s chief scientist Soumya Swaminathan, of Indian descent, tweeted out a reminder that ivermectin is not recommended to treat covid-19 patients. The tweet included a press release issued by the company that manufactures the drug, Merck, saying it had found no evidence to support the use of ivermectin in the treatment of COVID-19. Merck, it’s worth recalling, is developing an antiviral compound, molnupiravir, that will have to compete directly with ivermectin, one of the cheapest, safest drugs on the planet — unless, of course, ivermectin is taken out of the picture.
A Cautionary Tale
But if that happens, the result is likely to be a lot more deaths. Peru, the first country to use ivermectin against Covid, is living proof of that. The medicine was first used in eight states during the very early stages of the pandemic (May-July). After showing promise, it was extended to the whole country. Excess deaths dropped 59% (25%) at +30 days and 75% (25%) at +45 days after day of peak deaths. But in October, after the first wave had been brought under control, a newly elected government in Lima took the inexplicable step of withdrawing a number of medicines, including ivermectin, from its treatment guide for the disease.
Within weeks hospitalizations and deaths were soaring once again. The graph above, taken from a study by Juan Chamie, Jennifer Hibberd of the University of Toronto and David Scheim of the US Public Health Service, shows the sharp rise, fall and resurgence in excess deaths (among the over 60 year-old cohort) in Peru as the virus waxed, waned and waxed again. Since Peru dropped ivermectin the virus has raged through the population. Peru now has the highest per-capita death rate from covid on the planet. It’s a cautionary tale that India, with a population more than 30 times that of Peru, would do well to heed.
To be updated
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Graphene is the new asbestos. Plus injectable and mandatory. The rest Of the graphene oxide story is here, if you need more background, this post is a result of that investigation
NOTE: A needed clarification solicited by some readers: Yes, we knew of GRAPHENE COATING on masks in May, as seen below, which is horrible enough, even more so since not many followed Canada’s example in banning it. What this article brings new is a confirmation for GRAPHENE OXYDE, which is not very different in properties and health impact, but seems to be specific to these mRNA jabs, and so we complete the new revelations on graphene oxide and vaccines from La Quinta Columna.
In December 2019, a novel coronavirus (SARS-CoV-2) was first detected in Wuhan, in China’s Hubei province. On 11 March 2020, the World Health Organization (WHO) acknowledged and characterized the condition as a pandemic owing to the rapid spread of the virus across the globe infecting millions of individuals. Scientists are fighting tirelessly to find out ways to curb the spread of the virus and eradicate it.
SARS-CoV-2 is regarded as highly contagious and spreads rapidly through person-to-person contact. When an infected person sneezes or coughs, their respiratory droplets can easily infect a healthy individual. Besides enforcing social distancing, common citizens are encouraged to wear face masks to prevent droplets from getting through the air and infecting others.
Despite the efficiency of N95, a respiratory protective device, to filter out 95% of particles (≥0.3 μm), surgical facemasks are single-use, expensive, and often ill-fitting, which significantly reduces their effectiveness. Nanoscience researchers have envisioned a new respirator facemask that would be highly efficient, recyclable, customizable, reusable, and have antimicrobial and antiviral properties.
Nanotechnology in the Production of Surgical Masks
Nanoparticles are extensively used for their novel properties in various fields of science and technology.
In the current pandemic situation, scientists have adopted this technology to produce the most efficient masks. Researchers have used a novel electrospinning technology in the production of nanofiber membranes. These nanofiber membranes are designed to have various regulating properties such as fiber diameter, porosity ratio, and many other microstructural factors that could be utilized to produce high-quality face masks. Researchers in Egypt have developed face masks using nanotechnology with the help of the following components:
Polylactic acid
This transparent polymeric material is derived from starch and carbohydrate. It has high elasticity and is biodegradable. Researchers found that electrospun polylactic acid membranes possess high prospects for the production of filters efficient in the isolation of environmental pollutants, such as atmospheric aerosol and submicron particulates dispersed in the air.
Despite its various biomedical applications (implant prostheses, catheters, tissue scaffolds, etc.), these polylactic membranes are brittle. Therefore, applying frequent pressure during their usage could produce cracks that would make them permeable to viral particles. However, this mechanical drawback can be fixed using other supportive nanoparticles that could impart mechanical strength, antimicrobial and antiviral properties, which are important in making face masks effective in the current pandemic situation.
Copper oxide nanoparticles
These nanoparticles have many biomedical applications, for example, infection control, as they can inhibit the growth of microorganisms (fungi, bacteria) and viruses. It has also been reported that SARS-CoV-2 has lower stability on the metallic copper surface than other materials, such as plastic or stainless steel. Therefore, the integration of copper oxide nanoparticles in a nanofibrous polymeric filtration system would significantly prevent microbial adherence onto the membrane.
Graphene oxide nanoparticles
These nanoparticles possess exceptional properties, such as high toughness, superior electrical conductivity, biocompatibility, and antiviral and antibacterial activity. Such nanoparticles could be utilized in the production of masks.
Cellulose acetate
This is a semi-synthetic polymer derived from cellulose. It is used in ultrafiltration because of its biocompatibility, high selectivity, and low cost. It is also used in protective clothing, tissue engineering, and nanocomposite applications.
With the help of the aforesaid components, researchers in Egypt have designed a novel respirator filter mask against SARS-CoV-2. This mask is based on a disposable filter piece composed of the unwoven nanofibers comprising multilayers of a) copper oxide nanoparticles, graphene oxide nanoparticles, and polylactic acid, or b) copper oxide nanoparticles, graphene oxide nanoparticles, and cellulose acetate, with the help of electrospun technology and high-power ultrasonication. These facemasks are reusable, i.e., washable in water and could be sterilized using an ultraviolet lamp (λ = 250 nm).
SOURCE WORKING TO GET CONFIRMATION FROM THESE GUYS TOOSOURCE
Graphene-coated face masks: COVID-19 miracle or another health risk?
As a COVID-19 and medical device researcher, I understand the importance of face masks to prevent the spread of the coronavirus. So I am intrigued that some mask manufacturers have begun adding graphene coatings to their face masks to inactivate the virus. Many viruses, fungi and bacteria are incapacitated by graphene in laboratory studies, including feline coronavirus.
Because SARS CoV-2, the coronavirus that causes COVID-19, can survive on the outer surface of a face mask for days, people who touch the mask and then rub their eyes, nose, or mouth may risk getting COVID-19. So these manufacturers seem to be reasoning that graphene coatings on their reusable and disposable face masks will add some anti-virus protection. But in March, the Quebec provincial government removed these masks from schools and daycare centers after Health Canada, Canada’s national public health agency, warned that inhaling the graphene could lead to asbestos-like lung damage.
Is this move warranted by the facts, or an over-reaction? To answer that question, it can help to know more about what graphene is, how it kills microbes, including the SARS-COV-2 virus, and what scientists know so far about the potential health impacts of breathing in graphene.
How does graphene damage viruses, bacteria and human cells?
Graphene is a thin but strong and conductive two-dimensional sheet of carbon atoms. There are three ways that it can help prevent the spread of microbes:
Microscopic graphene particles have sharp edges that mechanically damage viruses and cells as they pass by them.
Graphene is negatively charged with highly mobile electrons that electrostaticly trap and inactivate some viruses and cells.
Dr Joe Schwarcz explains why Canada banned graphene masks. Doesn’t say why other countries didn’t. When two governments have opposing views on a poison, one is criminally wrong and someone has to pay.
Why graphene may be linked to lung injury
Researchers have been studying the potential negative impacts of inhaling microscopic graphene on mammals. In one 2016 experiment, mice with graphene placed in their lungs experienced localized lung tissue damage, inflammation, formation of granulomas (where the body tries to wall off the graphene), and persistent lung injury, similar to what occurs when humans inhale asbestos. A different study from 2013 found that when human cells were bound to graphene, the cells were damaged.
In order to mimic human lungs, scientists have developed biological models designed to simulate the impact of high concentration aerosolized graphene—graphene in the form of a fine spray or suspension in air—on industrial workers. One such study published in March 2020 found that a lifetime of industrial exposure to graphene induced inflammation and weakened the simulated lungs’ protective barrier.
It’s important to note that these models are not perfect options for studying the dramatically lower levels of graphene inhaled from a face mask, but researchers have used them in the past to learn more about these sorts of exposures. A study from 2016 found that a small portion of aerosolized graphene nanoparticles could move down a simulated mouth and nose passages and penetrate into the lungs. A 2018 study found that brief exposure to a lower amount of aerosolized graphene did not notably damage lung cells in a model.
From my perspective as a researcher, this trio of findings suggest that a little bit of graphene in the lungs is likely OK, but a lot is dangerous.
Although it might seem obvious to compare inhaling graphene to the well-known harms of breathing in asbestos, the two substances behave differently in one key way. The body’s natural system for disposing of foreign particles cannot remove asbestos, which is why long-term exposure to asbestos can lead to the cancer mesothelioma. But in studies using mouse models to measure the impact of high dose lung exposure to graphene, the body’s natural disposal system does remove the graphene, although it occurs very slowly over 30 to 90 days.
The findings of these studies shed light on the possible health impacts of breathing in microscopic graphene in either small or large doses. However, these models don’t reflect the full complexity of human experiences. So the strength of the evidence about either the benefit of wearing a graphene mask, or the harm of inhaling microscopic graphene as a result of wearing it, is very weak.
No obvious benefit but theoretical risk
Graphene is an intriguing scientific advance that may speed up the demise of COVID-19 virus particles on a face mask. In exchange for this unknown level of added protection, there is a theoretical risk that breathing through a graphene-coated mask will liberate graphene particles that make it through the other filter layers on the mask and penetrate into the lung. If inhaled, the body may not remove these particles rapidly enough to prevent lung damage.
The health department in Quebec is erring on the side of caution. Children are at very low risk of COVID-19 mortality or hospitalization, although they may infect others, so the theoretical risk from graphene exposure is too great. However, adults at high immediate risk of harm from contracting COVID-19 may choose to accept a small theoretical risk of long-term lung damage from graphene in exchange for these potential benefits.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Less decency and honesty in science than in politics, these days. I didn’t think there’s a few levels below politics.
You know when your juice bottle says “100% orange” and the small prints say it’s just 50% of fruit “concentrate”? They should be arrested for that. Now concentrate on this:
If I were to sum it up in words, I’d quote the source of this revelation:
“It is like saying that there were 700 men and 127 women studied and only a small percent got pregnant. Well, from the start 700 could not have gotten pregnant in the first place.”
Wheatley has just tipped LifeSite News on this, and I immediately did my own verification, anyone can and should do it. The result became the cover image for this article, which really is the beginning and the end of the debate, sums up Covidiocracy for me.
The data was collected and “arranged” by a team of “CDC experts” who published it in the New England Journal of Medicine in April 2021. It remained overlooked until mid July, when NEJM followed up with a shameless editorial that questioned nothing, just furthered the lie. And that’s when the small prints caught some diligent eyes and went to become our big headline today, as they deserve. Evil is in the small prints, again, that’s why they hate you when you carefully read inserts and labels.
This is Covidiocracy Science for you, this is the highly esteemed New England Journal of Medicine, up there, close to the British Medical Journal as reputation.
Mind that 82% is 3x the normal rate. All that extra dead babies blood is on the hands of CDC, NEJM and the likes of.
UPDATE:
A reader pointed out that Jeffrey Jaxxen too blew the lid on this, on Del Bigtree’s show, a few days back, and they reached precisely the same conclusion. BUT I noticed one very interesting detail that Del brought up and single-handedly proves intention in this fake narrative: The study hast no less than 54 authors. There is no chance in heaven and hell that they all missed this. If it’s not by mistake, it’s by intention.
This are just my highlights from the show, the full thing is linked above
And we really have to extrapolate this example to all walks of life, because they are all infected with the same corruption. None as blatantly as science, but you still can’t rely on anything you can’t research and verify yourself.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Sometimes my memes are 3D. And you can own them. Or send them to someone. You can even eat some of them. CLICK HERE
The Development, Concepts and Doctrine Centre (DCDC) has worked in partnership with the German Bundeswehr Office for Defence Planning to understand the future implications of human augmentation (HA), setting the foundation for more detailed Defence research and development.
The project incorporates research from German, Swedish, Finnish and UK Defence specialists to understand how emerging technologies such as genetic engineering, bioinformatics and the possibility of brain-computer interfaces could affect the future of society, security and Defence. The ethical, moral and legal challenges are complex and must be thoroughly considered, but HA could signal the coming of a new era of strategic advantage with possible implications across the force development spectrum.
HA technologies provides a broad sense of opportunities for today and in the future. There are mature technologies that could be integrated today with manageable policy considerations, such as personalised nutrition, wearables and exoskeletons. There are other technologies in the future with promises of bigger potential such as genetic engineering and brain-computer interfaces. The ethical, moral and legal implications of HA are hard to foresee but early and regular engagement with these issues lie at the heart of success.
HA will become increasingly relevant in the future because it is the binding agent between the unique skills of humans and machines. The winners of future wars will not be those with the most advanced technology, but those who can most effectively integrate the unique skills of both human and machine.
The growing significance of human-machine teaming is already widely acknowledged but this has so far been discussed from a technology-centric perspective. This HA project represents the missing part of the puzzle.
Disclaimer
The content of this publication does not represent the official policy or strategy of the UK government or that of the UK’s Ministry of Defense (MOD).
Furthermore, the analysis and findings do not represent the official policy or strategy of the countries contributing to the project.
It does, however, represent the view of the Development, Concepts and Doctrine Centre (DCDC), a department within the UK MOD, and Bundeswehr Office for Defence Planning (BODP), a department within the German Federal Ministry of Defence. It is based on combining current knowledge and wisdom from subject matter experts with assessments of potential progress in technologies 30 years out supporting deliberations and deductions for future humans and society. Published 13 May 2021 – UK DEFENSE WEBSITE
That disclaimer is a load of bollocks that means nothing, really, but covers the Ministry from some legal liabilities, just in case. You can totally ignore it. – Silview.media
The US Department of Defense has something similar going on, but it doesn’t target the general population in presentations. However, if you input “DARPA” in our search utility, you find out DoD has been going same direction for decades.
At least US has the decency to pretend these are for military use only, I know they all are meant to be used on the general population, but I don’t know any other open admission of civillian use before.
Does this guy shock you that much now, or does he fall in line like the perfect Tetris piece that he is, “another brick in the wall”?
Now remember mRNA therapies are “information therapies” and these injections are the perfect tools for achieving the above goals.
Anyone remember the plebs ever being consulted on their future evolution, or are they just SUBJECTED to it, like slaves to selective breeding?!
You read this because some of my readers are generous enough to help us survive, and at least as hungry for truth as we are, basically the best readers I could hope for. Such as Corinne, who we should thank for pulling my sleeve about this one! If you’re on Gab (which you should), follow her, she has tons of great info to share every day!
DEVELOPING STORY, TO BE CONTINUED, SO BE BACK HERE SOON
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them