Never believe what we say, always research what we say. As for CDC, if you research what they say you end up finding out they have 85% failure rates.
This is the recent CDC report, in PDF format, sourced from the CDC website. And below is my sufficient commentary in visual form. There’s nothing else to say, the official narrative is dead and buried, at this point we’re just burning calories if we keep flogging it.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Companies collecting data for pubs and restaurants to help them fulfil their contact-tracing duties are harvesting confidential customer information to sell.
Legal experts have warned of a “privacy crisis” caused by a rise in companies exploiting QR barcodes to take names, addresses, telephone numbers and email details, before passing them on to marketers, credit companies and insurance brokers.
The “quick response” mobile codes have been widely adopted by the hospitality, leisure and beauty industries as an alternative to pen-and-paper visitor logs since the government ordered businesses to collect contact details to give to NHS Test and Trace if required.
Any data collected should be kept by the business for 21 days and must not be used “for any purposes other than for NHS Test and Trace”, according to government guidelines.
But some firms used by businesses to meet the new requirements have clauses in their terms and conditions stating they can use the information for reasons other than contact tracing, including sharing it with third parties. The privacy policy of one company used by a restaurant chain in London says it stores users’ data for 25 years.
Gaurav Malhotra, director of Level 5, a software development company that supplies the government, said data could end up in the hands of scammers. “If you’re suddenly getting loads of texts, your data has probably been sold on from track-and-trace systems,” he said.
One of the firms claiming to offer a privacy-compliant QR code service is Pub Track and Trace (PUBTT), an organisation based in Huddersfield charging pubs £20 a month to keep track of visitors, who are asked to provide their name, phone number and email address.
Despite its claim to be a “simple” service, its privacy policy, which users must accept, explains how personal data of people accessing its website can be used to “make suggestions and recommendations to you about goods or services that may be of interest to you” and shared with third parties including “service providers or regulatory bodies providing fraud prevention services or credit/background checks.”
It may also “collect, use, store and transfer” records of access to certain premises including “time, ID number and CCTV images”.
PUBTT, which works with pubs in England and Wales, said users agreed to its privacy policy before using the service and claimed it had not passed data to third parties. A spokesman, identified only as Adam H, said: “The data we collect is only for use of the Test and Trace service or where a user has agreed for the venue to use their information for marketing purposes.”
Ordamo, which provides track and trace services for restaurants, states that data from website visitors is “retained for 25 years”, a duration Hazel Grant, head of privacy at Fieldfisher, a law firm, said would be “very difficult to justify”. Ordamo did not respond to requests for comment.
The Information Commissioner’s Office is assessing 15 companies that “provide services to venues to collect customer logs”.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
This just happened. And much more. As we’ve warned you since March, but people thought WHO can take better care of them. OK then…
It’s World Mental Health Day! -Close to 1 billion people have a mental disorder -Depression is a leading cause of illness & disability -1 person dies every 40 seconds from suicide -3 million people die every year due to harmful use of 🍻#MoveForMentalHealth: Let’s invest!
“Very sadly, more boys under the age of 18 in nine-months alone, than we’ve ever seen in Victoria over a full 12-month period have taken their life this year,”
Per coincidence as ever, the suicide rates among Victoria’s teenagers are up over 30% this year, just like among US Army soldiers. I wonder what they had in common, right?
Army active-duty suicides are up 30% during the same time frame as COVID-19.
These “meh people” are the same ones who loudly and aggressively act as if they are entitled to free heaith care (mask-wearing) from their victims. How about some warm flegm instead?
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
For most of its history, GSK has been headed by the current “US Vaccine Czar“, the head of Operation Warp Speed, Moncef Slaoui, handpicked by Jared Kushner in Trump’s name.
If anyone claims it’s not good, how could’ve they known that in Februaty or in March, when the virus was “novel” and “the data was scarce”?
Can we expect to find more examples of either drug patents that don’t work or hidden medical and science advancements, whatever the case might be here?
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
by James T. Keane, Originally published by American Magasine on May 12, 2020
Dr. Anthony Fauci meets with New York City’s Regis High School students and the school’s president, Daniel Lahart, S.J., in 2019. (CNS photo/courtesy Regis High School)
We’ve just unearthed a message distributed earlier in May 2020 by Dr. Anthony Fauci, M.D., the director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health and a leading figure in the struggle to contain the coronavirus pandemic, addressed the graduating classes of 2020 at Jesuit secondary schools around the country.
Dr. Fauci testified via video before the Senate Committee on Health, Education, Labor and Pensionson Tuesday. He is observing a “modified quarantine” after coming into contact with a White House staffer who tested positive for the coronavirus.
“Currently our lives have been upended by a truly historic global pandemic. I am profoundly aware that graduating during this time—and virtually, without your friends, classmates and teachers close by—is extremely difficult,” Dr. Fauci said. “However, please hang in there. We need you to be smart, strong and resilient. With discipline and empathy, we will all get through this together.”
The video originated with a request from Daniel Lahart, S.J., president of Regis High School in New York, Dr. Fauci’s alma mater, that Dr. Fauci record a short address to the school’s graduating class. “Like most schools, we won’t be gathering in June for our usual graduation exercises,” Father Lahart told America. “As a staff, we have talked a great deal about how to mark our graduation day as special. Another Zoom just doesn’t do it.”
After another Jesuit, Jeff Johnson, S.J., president of Strake Jesuit College Preparatory in Houston (where Father Lahart was previously president), mentioned that he had a similar idea, Father Lahart contacted Dr. Fauci’s office and asked if he could do a second video that was not specific to Regis, and that could be shared with other Jesuit high schools. “It was an audacious ask of someone who is incredibly busy, and concerned with worldwide health,” Father Lahart commented. “But he speaks so easily about what his Jesuit education means to him, so I presumed it wouldn’t take him long to film either one.”
“Every Jesuit graduate can take pride in knowing that they are part of an educational system that is nearly five centuries old, and has impacted the lives or so many people around the world,” Father Lahart continued. “Today, we also can all take pride that the man who is probably the most trusted person in the United States is a graduate of a Jesuit high school and a Jesuit college. He takes great pride in his Jesuit education, and as he proudly professes, it has formed his life and his career.”
“We can all take pride that the man who is probably the most trusted person in the United States is a graduate of a Jesuit high school and a Jesuit college.”
Dr. Fauci was born in the Bensonhurst section of Brooklyn in 1940 and graduated from Regis High School in 1958. Applicants to the all-male Jesuit school were expected to be among the top students in their graduating class and took a rigorous entrance exam. Enrollment was kept at 140 students per class year. The school was founded in 1914 with a substantial financial gift from Julia M. Grant, the widow of New York City Mayor Hugh J. Grant. Terms of the endowment included that the school charge its students no tuition, a policy still in place today.
“I often say it was the best educational experience I could have imagined,” Dr. Fauci noted in his speech. “I became immersed in the intellectual rigor of a Jesuit education.”
Tom McCorry, a classmate of Dr. Fauci who also played with him on the Regis basketball team (Dr. Fauci was team captain in 1958) and later went on to become a college basketball coach, told America that Regis “was a very high-end academic school, just as Jesuit education in general is very high-end. We took four years of Latin, four years of Greek and a couple of years or French or German. It was quite a school, but Tony [Fauci] stood out in a number of ways.”
“He was very astute, quiet but a leader,” Mr. McCorry remembered. “He still shows it now. When all these things get thrown at him [during White House press briefings], you don’t see him losing his temper. You see him give measured answers based on the facts.”
Dr. Fauci graduated from The College of the Holy Cross in 1962, and received his medical doctorate from the Weill Medical College of Cornell University in 1966. He has served under six U.S. presidents, starting with Ronald Reagan in 1984. He noted in a 2019 visit to Regis that he was able to work under different presidential administrations because “I am almost completely apolitical.” Widely considered the top infectious disease expert in the United States, Dr. Fauci has worked on the federal response to AIDS, Zika, anthrax and Ebola, and is currently a member of the White House coronavirus task force. In 2008, Dr. Fauci was awarded the Presidential Medal of Freedom.
Dr. Fauci credited his education at Regis High School with teaching him both “precision of thought and economy of expression.”
Dr. Fauci credited his education at Regis with teaching him both “precision of thought and economy of expression,” commenting that those two habits “inform how I think, how I write and how I communicate with the public every day, especially during the present unsettling times. Just as important, however, is the Jesuit emphasis on social justice and service to others. And now is the time, if ever there was one, for us to care selflessly about one another.”
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Sometimes my memes are 3D. And you can own them. Or send them to someone. You can even eat some of them. CLICK HERE
The infamous Knights Templar has elected a new master in January 2020. We’ve just discovered he officially endorsed Donald Trump’s 2020 re-election as POTUS. For anyone who has at least a superficial knowledge of the Templar history and power, the implications are bigger than big.
Can’t vouch for the Internet-famous Structure of Masonry, but this is cut from it and pretty accurate for a memeFull screen
In a new joint letter released 15th of September 2020, 235 senior military leaders officially endorsed President Donald Trump’s reelection.
“The 2020 election affords the American people an urgently needed opportunity to affirm their devotion to the Constitution of the United States and to the American way of life. As senior leaders of America’s military, we took an oath to defend the United States from all enemies, foreign and domestic. At present, our country is now confronted with enemies here and abroad, as well as a once in a century pandemic,” the letter says. “As retired military officers, we believe that Donald J. Trump has been tested as few other presidents have and is the proven leader to confront these dangers.”
According to American Military News, the letter, which is signed by eight four-star generals/admirals, 42 three-star generals/admirals, goes on to call the 2020 presidential election the most important since the United States’ inception. It names off threats such as socialism and Marxism, and defense spending cuts as some of the most detrimental to Americans’ security and way of life.
“The proposed defense cuts by the Democrats will, in our professional judgment, create a potentially perilous situation for the United States during a time of great external and internal threats to our Nation,” the letter adds.
The letter also takes aim at Biden, criticizing him and former President Obama for harming military strength through “a series of ill-considered and debilitating budget cuts” during their administration.
“For these reasons, we support Donald Trump’s re-election. We believe that President Donald Trump is committed to a strong America. As president, he will continue to secure our borders, defeat our adversaries, and restore law and order domestically,” the letter says. “We urge our fellow Americans to join us in supporting the re-election of Donald Trump for President.”
Read the full text of the letter below:
Open Letter from Senior Military Leaders The 2020 election affords the American people an urgently needed opportunity to affirm their devotion to the Constitution of the United States and to the American way of life. As senior leaders of America’s military, we took an oath to defend the United States from all enemies, foreign and domestic. At present, our country is now confronted with enemies here and abroad, as well as a once in a century pandemic. As retired military officers, we believe that Donald J. Trump has been tested as few other presidents have and is the proven leader to confront these dangers.
It can be argued that this is the most important election since our country was founded. With the Democratic Party welcoming to socialists and Marxists, our historic way of life is at stake.
During the Obama/Biden administration, America’s armed forces were subjected to a series of ill-considered and debilitating budget cuts. The Democrats have once again pledged to cut defense spending, undermining our military strength.
The Democrats’ opposition to border security, their pledge to return to the disastrous Iran nuclear deal, their antagonism towards the police and planned cuts to military spending will leave the United States more vulnerable to foreign enemies.
President Trump’s resolute stands have deterred our enemies from aggression against us and our allies. The proposed defense cuts by the Democrats will, in our professional judgment, create a potentially perilous situation for the United States during a time of great external and internal threats to our Nation.
For these reasons, we support Donald Trump’s re-election. We believe that President Donald Trump is committed to a strong America. As president, he will continue to secure our borders, defeat our adversaries, and restore law and order domestically.
We urge our fellow Americans to join us in supporting the re-election of Donald Trump for President.
Plenty of interesting characters on that list of signatures, but one picked up our attention more than others: Brig. General Ronald S. Mangum. Because of earlier news from January:
Brig. General Ronald S. Mangum elected as the new Master of the Ordre Souverain et Militaire du Temple de Jerusalem
Brig. Gen. Ronald S. Mangum, Master OSMTJ
After a long absence the office of Master for the OSMTJ, better known as the Knights Templar, has finally been filled. Brigadier General Ronald S. Mangum acknowledge the accolade with the following letter:
Dear Templar brothers and sisters – I am deeply honored that you have selected me to fill the long vacate office of Master of the Ordre Souverain et Militaire du Temple de Jerusalem. I did not initiate this action, but I will accept the will of the Grand Priors and will serve the Order to the best of my ability. We are an ancient and noble Christian Order and we have much work ahead to do to fulfil our ecumenical and humanitarian role in today’s world. Again, thank you for your confidence in me, and may God bless our Order.
Message For Everyone From Newly Elected International Master of OSMTJ Knights Templar, Brig. General Ronald S. Mangum
“We warmly welcome to our Leadership, this exceptionally accomplished and long-time Templar legend. Joining in 1995, General Mangum has been a Templar leader for 21 years and brings the incredible breadth and width of his experience to bear for the OSMTJ International (OSMTJ.net). General Mangum has served in many of the highest Templar Positions over the years, the Deputy Grand Commander of the OSMTH.org, a Grand Prior in Austria for that same order, a Grand Preceptor in the nation of Georgia (he practically created the Grand Priory of Georgia), and many other roles.
Master of the Order, General Ronald Mangum Knighting members in the nation of Georgia
As a practicing lawyer, Attorney Mangum was admitted to practice before the Supreme Courts of Illinois (1968) and Wisconsin (1985), the United States Tax Court, the United States Supreme Court, the United States Court of Appeals for the Seventh Circuit, the United States District Courts (Northern, Central and Southern Districts of Illinois) and the Federal Trial Bar.[3] Mangum practised law in Chicago for over 30 years, founding the firm of Mangum, Smietanka & Johnson, L.L.C. He served in several leadership positions in the Illinois State Bar Association and the Chicago Bar Association.
As a Professor, Ronald Mangum served as a full Professor of National Security Studies from 2005 to 2011 at American Military University and briefly served as Program Director of the National Security Studies Program in 2006. He developed and taught courses in Research Methods in National Security Studies, Concepts of National Security, U.S. National Security, International Security, Diplomacy and National Security and Institutions of National Security.
Master of the OSMTJ Order, General Ronald Mangum in Georgia
As for his military career, General Mangum retired from the United States Army in November 2004 after 35 years of enlisted and officer service. His last command consisted of three elements: Commanding General, Special Operations Command Korea; Commanding General, United Nations Special Operations Component; and Deputy Commanding General, Combined Unconventional Warfare Task Force. He served in Korea from September 2000 to August 2003.
Previous command assignments included Deputy Division Commander; Assistant Division Commander (Logistics); Commander, 1st Brigade (Battle Command Staff Training); Commander, 4th Brigade (Field Exercise Training); Commander, Battle Projection Group (Battle Command Staff Training); Commander, 1st Battalion, 340th Regiment (Instructor); all in the 85th Division (Training Support).[2] He also served as the Operations Officer (S-3) of the 314th Army Security Agency Battalion, Group Intelligence Officer (S-2) and Commander, Operational Detachment A, 1st Battalion, 12th Special Forces Group (Airborne), Arlington Heights, Illinois.
His military awards include the Distinguished Service Medal, Defense Superior Service Medal, Meritorious Service Medal, Joint Service Commendation Medal, Army Commendation Medal with one silver and two bronze oak leaf clusters, and the Order of Cheong Su (Republic of Korea), among others. His military qualifications include the Ranger Tab, Master Parachutist badges (U.S. and Republic of Korea), Pathfinder Badge, Special Operations Diver badge, Aircrew Badge and Canadian Parachutist badge. General Mangum’s military education included the Infantry Officer Basic and Advanced courses, Special Forces Qualification Course, Military Intelligence Officer Advanced Course, Civil Affairs Officer Advanced Course, Engineer Officer Advanced Course, the United States Army Command and General Staff Course, the United States Army War College, Capstone and the Joint General Officer/Flag Officer Warfighters Course. Following his retirement from military service, he became a consultant to the United States Department of Defense and was contracted as a senior advisor to the Georgian Ministry of Defense from 2005 to 2011.
This is as new as October 2020 and might be the only video recording of his available on Internet
BONUS: Mangum was also a co-signer of the letter that bashed NBC for bashing Navy SEAL sniper Chris Kyle. So I guess he’s involved with a nucleus of elder military who share his convictions. Don’t be surprised if many share more than just convictions.
ALSO: If any of his distinguished colleagues reads this, please notify Mangum and everyone that you have a rogue element in your organization, a total Hillary shill lol, read here
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Aleksandr Cassandra Rockefeller, or simply Aleksandra Rockefeller has been for a long time a kind of myth to me and many underground truthers that went far enough down the rabbit hole. On Internet, she is usually portrayed like a dark shadowy female villain in a 007 movie, too spectacular to be true, I naively thought. Because one of her first names sounds masculine to Westerners (common in Russia), many have doubts she’s even a woman, some assume it’s a couple acting under one alias or something of that sort. Not my kind of mystery, to be hones, so I’ve never looked into it. Until recently, when I was investigating her clan, one link led to another and I managed to trace her and , bwoyyy!, her Facebook profile. What I found is spectacular beyond her fame!
Born: Netherlands Birth date: Unknown Official birth name: Schuman (only one source, needs more) Political affiliations: former Clinton fanatic, currently wishing all the best to Trump (see slideshow below)
Here she is sending best wishes to some poor bastard stalking her on Facebook
So the character is otherwise quite hard to detect on internet, but she’s verified and legit. I won’t link directly to her Facebook for protection reasons, and I can’t recommend any action besides seeing what’s public there, for own education. Below there are some fine digs and I’ll have some more exclusive info soon, working to get solid background for it. Our fate depends, now more than ever, on understanding the webs of deep state, which is trans-national, its patrons don’t have just a country, but dozens. Their “patriae” (home-country) is ideological and often genetic.
My greatest curiosity about her is how she finds balance between her love for Hillary, her duties for the US government and her duties for the Knights Templar, whose new master officially endorses Trump.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
It’s not disputable, since the information comes from official patent registries in the Netherlands and US. And we have all the documentation
UPDATE: Reuters took on doing damage control for this article and published a slander and smear piece on us disguised as “fact-checking”. We fact-checked their fact-checking phrase by phrase here.
As we’ve shown in previous exposes, the whole Covidiocracy is a masquerade and a simulation long prepared by The World Bank / IMF / The Rothschilds and their lemmings, with Rockefeller partnership. Our newest discoveries further these previous revelations.
A method is provided for acquiring and transmitting biometric data (e.g., vital signs) of a user, where the data is analyzed to determine whether the user is suffering from a viral infection, such as COVID-19. The method includes using a pulse oximeter to acquire at least pulse and blood oxygen saturation percentage, which is transmitted wirelessly to a smartphone. To ensure that the data is accurate, an accelerometer within the smartphone is used to measure movement of the smartphone and/or the user. Once accurate data is acquired, it is uploaded to the cloud (or host), where the data is used (alone or together with other vital signs) to determine whether the user is suffering from (or likely to suffer from) a viral infection, such as COVID-19. Depending on the specific requirements, the data, changes thereto, and/or the determination can be used to alert medical staff and take corresponding actions.
Title: System and Method for Using, Biometric, and Displaying Biometric Data United States Patent Application 20170229149 Kind Code: A1
Abstract: A method is provided for processing and displaying biometric data of a user, either alone or together (in synchronization) with other data, such as video data of the user during a time that the biometric data was acquired. The method includes storing biometric data so that it is linked to an identifier and at least one time-stamp (e.g., a start time, a sample rate, etc.), and storing video data so that it is linked to the identifier and at least one time-stamp (e.g., a start time). By storing data in this fashion, biometric data can be displayed (either in real-time or delayed) in synchronization with video data, and biometric data can be searched to identify at least one biometric event. Video corresponding to the biometric event can then be displayed, either alone or together with at least one biometric of the user during the biometric event.
Inventors: Rothschild, Richard A. (London, GB) Macklin, Dan (Stafford, GB) Slomkowski, Robin S. (Eugene, OR, US) Harnischfeger, Taska (Eugene, OR, US) Application Number: 15/495485 Publication Date: 08/10/2017 Filing Date: 04/24/2017 Export Citation: Click for automatic bibliography generation Assignee: Rothschild Richard A. Macklin Dan Slomkowski Robin S. Harnischfeger Taska International Classes: G11B27/10; G06F19/00; G06K9/00; G11B27/031; H04N5/77 View Patent Images: Download PDF 20170229149
US Patent References:
20160035143
N/A
2016-02-04
20140316713
N/A
2014-10-23
20140214568
N/A
2014-07-31
20090051487
N/A
2009-02-26
20070189246
N/A
2007-08-16
Primary Examiner: MESA, JOSE M Attorney, Agent or Firm: Fitzsimmons IP Law (Gardena, CA, US) Claims: What is claimed is:
1. A method for identifying video corresponding to a biometric event of a user, said video being displayed along with at least one biometric of said user during said biometric event, comprising: receiving a request to start a session; using at least one program running on a mobile device to assign a session number and a start time to said session; receiving video data from a camera, said video data including video of at least one of said user and said user’s surroundings during a period of time, said period of time starting at said start time; receiving biometric data from a sensor, said biometric data including a plurality of values on a biometric of said user during said period of time; using said at least one program to link at least said session number and said start time to said video data; using said at least one program to link at least said session number, said start time, and a sample rate to said biometric data, at least said session number being used to link said biometric data to said video data, and at least said sample rate and said start time being used to link individual ones of said plurality of values to individual times within said period of time; receiving said biometric event, said biometric event comprising one of a value and a range of said biometric; using said at least one program to identify a first one of said plurality of values corresponding to said biometric event; using said at least one program and at least said start time, said sample rate, and said period of time to identify a first time within said period of time corresponding to said first one of said plurality of values; and displaying on said mobile device at least said video data during said first time along with said first one of said plurality of values, wherein said first time is used to show said first one of said plurality of values in synchronization with a portion of said video data that shows at least one of said user and said user’s surroundings during said biometric event.
2. The method of claim 1, wherein said step of receiving biometric data from said sensor further comprises receiving heart rate data from a heart rate monitor.
3. The method of claim 1, wherein said steps of linking said session number to said video data and said biometric data further comprises linking an activity number to both said video data and said biometric data, wherein said activity number identifies one of a plurality of activities, said session comprises said plurality of activities, and both said session number and said activity number are used to link said biometric data to said video data.
4. The method of claim 1, wherein said step of assigning a session number to said session further comprises linking a description of said session to said session.
5. The method of claim 1, wherein said steps of receiving video data and biometric data further comprises receiving said video data and said biometric data during said period of time.
6. The method of claim 1, wherein said step of receiving video data from a camera further comprises receiving said video data from said camera after said period of time.
7. The method of claim 6, further comprising the step of analyzing said video data for an identifier identifying said session, said identifier being used by said at least one program to link said session number to said video data.
8. The method of claim 1, wherein said steps of identifying a first one of said plurality of values corresponding to said biometric event and identifying a first time corresponding to said first one of said plurality of values further comprises identifying each one of said plurality of values corresponding to said biometric event and identifying each time corresponding to said each one of said plurality of values.
9. The method of claim 8, wherein said step of displaying at least said video data during said first time further comprises displaying at least said video data during said each time corresponding to said each one of said plurality of values, wherein said each time is used to show said each one of said plurality of values in synchronization with portions of said video data that show at least one of said user and said user’s surroundings during said biometric event.
10. The method of claim 1, further comprising the steps of receiving self-realization data from said user, and linking at least said session number and at least one time to said self-realization data, wherein said self-realization data indicates how said user feels during said at least one time, and said at least one time is used to display said self-realization data in synchronization with at least one portion of said video data.
11. A system for identifying video corresponding to a biometric event of a user, said video being displayed along with at least one biometric of said user during said biometric event, comprising: at least one server in communication with a wide area network (WAN); a mobile device in communication with said at least one server via said WAN, said mobile device comprising: a display; at least one processor for downloading machine readable instructions from said at least one server; and at least one memory device for storing said machine readable instructions, said machine readable instructions being adapted to perform the steps of: receiving a request to start a session; assigning a session number and a start time to said session; receiving video data from a camera, said video data including video of at least one of said user and said user’s surroundings during a period of time; receiving biometric data from a sensor, said biometric data including a plurality of values on a biometric of said user during said period of time; linking at least said session number and said start time to said video data; linking at least said session number, said start time, and a sample rate to said biometric data, at least said session number being used to link said biometric data to said video data, and at least said sample rate and said start time being used to link individual ones of said plurality of values to individual times within said period of time; receiving said biometric event, said biometric event comprising one of a value and a range of said biometric; identifying a first one of said plurality of values corresponding to said biometric event; identifying a first time within said period of time corresponding to said first one of said plurality of values; and displaying on said display at least said video data during said first time along with said first one of said plurality of values, wherein said first time is used to show said first one of said plurality of values in synchronization with a portion of said video data that shows at least one of said user and said user’s surroundings during said biometric event.
12. The system of claim 11, wherein said step of receiving biometric data from said sensor further comprises receiving heart rate data from a heart rate monitor.
13. The system of claim 11, wherein said steps of linking said session number to said video data and said biometric data further comprises linking an activity number to both said video data and said biometric data, wherein said activity number identifies one of a plurality of activities, said session comprises said plurality of activities, and both said session number and said activity number are used to link said biometric data to said video data.
14. The system of claim 11, wherein said steps of receiving video data and biometric data further comprises receiving said video data and said biometric data during said period of time.
15. The system of claim 11, wherein said step of receiving video data from a camera further comprises receiving said video data from said camera after said period of time.
16. The system of claim 15, wherein said machine readable instructions are further adapted to perform the step of analyzing said video data for a barcode, said barcode identifying said session number and being used to link said session number to said video data.
17. The system of claim 11, wherein said steps of identifying a first one of said plurality of values corresponding to said biometric even and identifying a first time corresponding to said first one of said plurality of values further comprises identifying each one of said plurality of values corresponding to said biometric event and identifying each time corresponding to said each one of said plurality of values.
18. The system of claim 17, wherein said step of displaying at least said video data during said first time further comprises displaying at least said video data during said each time corresponding to said each one of said plurality of values, wherein said each time is used to show said each one of said plurality of values in synchronization with portions of said video data that show at least one of said user and said user’s surroundings during said biometric event.
19. The system of claim 11, wherein said machine readable instructions are further adapted to perform the steps of receiving self-realization data from said user, and linking said session number and at least one time to said self-realization data, wherein said self-realization data indicates how said user feels during said at least one time, and said at least one time is used to display said self-realization data in synchronization with at least one portion of said video data.
20. A method for displaying video in synchronization with at least one biometric of a subject, comprising: using at least one program running on a computing device to assign a session number and a start time to said session; receiving video data from at least one camera, said video data including video of at least one of said subject and said subject’s surroundings during a period of time; receiving biometric data from at least one sensor, said biometric data including a plurality of values on at least one biometric of said subject during said period of time; using said at least one program to link at least said session number and said start time to said video data; using said at least one program to link at least said session number, said start time, and at least one sample rate to said biometric data; receiving a biometric event, said biometric event comprising one of a value and a range of said at least one biometric; using said at least one program to identify individual ones of said plurality of values corresponding to said biometric event; using said at least one program and at least said start time, said at least one sample rate, and said period of time to identify individual times within said period of time corresponding to said individual ones of said plurality of values; and displaying on said computing device at least said video data and said individual ones of said plurality of values, wherein said individual times are used to show said individual ones of said plurality of values in synchronization with portions of said video data that show at least one of said subject and said subject’s surroundings during said biometric event.
Description:
CROSS-REFERENCE TO RELATED APPLICATION
This application is a continuation of Ser. No. 15/293,211, filed Oct. 13, 2016, which claims priority pursuant to 35 U.S.C. §119 (e) to U.S. Provisional Application No. 62/240,783, filed Oct. 13, 2015, which applications are specifically incorporated herein, in their entirety, by reference.
BACKGROUND OF THE INVENTION
1. Field of the Invention
The present invention relates to the reception and use of biometric data, and more particularly, to a system and method for displaying at least one biometric of a user along with video of the user at a time that the at least one biometric is being measured and/or received.
2. Description of Related Art
Recently, devices have been developed that are capable of measuring, sensing, or estimating in a convenient form factor at least one or more metric related to physiological characteristics, commonly referred to as biometric data. For example, devices that resemble watches have been developed which are capable of measuring an individual’s heart rate or pulse, and, using that data together with other information (e.g., the individual’s age, weight, etc.), to calculate a resultant, such as the total calories burned by the individual in a given day. Similar devices have been developed for measuring, sensing, or estimating other kinds of metrics, such as blood pressure, breathing patterns, breath composition, sleep patterns, and blood-alcohol level, to name a few. These devices are generically referred to as biometric devices or biosensor metrics devices.
While the types of biometric devices continue to grow, the way in which biometric data is used remains relatively static. For example, heart rate data is typically used to give an individual information on their pulse and calories burned. By way of another example, blood-alcohol data is typically used to give an individual information on their blood-alcohol level, and to inform the individual on whether or not they can safely or legally operate a motor vehicle. By way of yet another example, an individual’s breathing pattern (measurable for example either by loudness level in decibels, or by variations in decibel level over a time interval) may be monitored by a doctor, nurse, or medical technician to determine whether the individual suffers from sleep apnea.
While biometric data is useful in and of itself, such data would be more informative or dynamic if it could be combined with other data (e.g., video data, etc.), provided (e.g., wirelessly, over a network, etc.) to a remote device, and/or searchable (e.g., allowing certain conditions, such as an elevated heart rate, to be quickly identified) and/or cross-searchable (e.g., using biometric data to identify a video section illustrating a specific characteristic, or vice-versa). Thus, a need exists for an efficient system and method capable of achieving at least some, or indeed all, of the foregoing advantages, and capable also of merging the data generated in either automatic or manual form by the various devices, which are often using operating systems or technologies (e.g., hardware platforms, protocols, data types, etc.) that are incompatible with one another.
In certain embodiments of the present invention, the system and/or method is configured to receive, manage, and filter the quantity of information on a timely and cost-effective basis, and could also be of further value through the accurate measurement, visualization (e.g., synchronized visualization, etc.), and rapid notification of data points which are outside (or within) a defined or predefined range.
Such a system and/or method could be used by an individual (e.g., athlete, etc.) or their trainer, coach, etc., to visualize the individual during the performance of an athletic event (e.g., jogging, biking, weightlifting, playing soccer, etc.) in real-time (live) or afterwards, together with the individual’s concurrently measured biometric data (e.g., heart rate, etc.), and/or concurrently gathered “self-realization data,” or subject-generated experiential data, where the individual inputs their own subjective physical or mental states during their exercise, fitness or sports activity/training (e.g., feeling the onset of an adrenaline “rush” or endorphins in the system, feeling tired, “getting a second wind,” etc.). This would allow a person (e.g., the individual, the individual’s trainer, a third party, etc.) to monitor/observe physiological and/or subjective psychological characteristics of an individual while watching or reviewing the individual in the performance of an athletic event, or other physical activity. Such inputting of the self-realization data, ca be achieved by various methods, including automatically, time-stamped-in-the-system voice notes, short-form or abbreviation key commands on a smart phone, smart watch, enabled fitness band, or any other system-linked input method which is convenient for the individual to utilize so as not to impede (or as little as possible) the flow and practice by the individual of the activity in progress.
Such a system and/or method would also facilitate, for example, remote observation and diagnosis in telemedicine applications, where there is a need for the medical staff, or monitoring party or parent, to have clear and rapid confirmation of the identity of the patient or infant, as well as their visible physical condition, together with their concurrently generated biometric and/or self-realization data.
Furthermore, the system and/or method should also provide the subject, or monitoring party, with a way of using video indexing to efficiently and intuitively benchmark, map and evaluate the subject’s data, both against the subject’s own biometric history and/or against other subjects’ data samples, or demographic comparables, independently of whichever operating platforms or applications have been used to generate the biometric and video information. By being able to filter/search for particular events (e.g., biometric events, self-realization events, physical events, etc.), the acquired data can be reduced down or edited (e.g., to create a “highlight reel,” etc.) while maintaining synchronization between individual video segments and measured and/or gathered data (e.g., biometric data, self-realization data, GPS data, etc.). Such comprehensive indexing of the events, and with it the ability to perform structured aggregation of the related data (video and other) with (or without) data from other individuals or other relevant sources, can also be utilized to provide richer levels of information using methods of “Big Data” analysis and “Machine Learning,” and adding artificial intelligence (“AI”) for the implementation of recommendations and calls to action.
SUMMARY OF THE INVENTION
The present invention provides a system and method for using, processing, indexing, benchmarking, ranking, comparing and displaying biometric data, or a resultant thereof, either alone or together (e.g., in synchronization) with other data (e.g., video data, etc.). Preferred embodiments of the present invention operate in accordance with a computing device (e.g., a smart phone, etc.) in communication with at least one external device (e.g., a biometric device for acquiring biometric data, a video device for acquiring video data, etc.). In a first embodiment of the present invention, video data, which may include audio data, and non-video data, such as biometric data, are stored separately on the computing device and linked to other data, which allows searching and synchronization of the video and non-video data.
In one embodiment of the present invention, an application (e.g., running on the computing device, etc.) includes a plurality of modules for performing a plurality of functions. For example, the application may include a video capture module for receiving video data from an internal and/or external camera, and a biometric capture module for receiving biometric data from an internal and/or external biometric device. The client platform may also include a user interface module, allowing a user to interact with the platform, a video editing module for editing video data, a file handling module for managing data, a database and sync module for replicating data, an algorithm module for processing received data, a sharing module for sharing and/or storing data, and a central login and ID module for interfacing with third party social media websites, such as Facebook™.
These modules can be used, for example, to start a new session, receive video data for the session (i.e., via the video capture module) and receive biometric data for the session (i.e., via the biometric capture module). This data can be stored in local storage, in a local database, and/or on a remote storage device (e.g., in the company cloud or a third-party cloud service, such as Dropbox™, etc.). In a preferred embodiment, the data is stored so that it is linked to information that (i) identifies the session and (ii) enables synchronization.
For example, video data is preferably linked to at least a start time (e.g., a start time of the session) and an identifier. The identifier may be a single number uniquely identifying the session, or a plurality of numbers (e.g., a plurality of global or universal unique identifiers (GUIDs/UUIDs)), where a first number uniquely identifying the session and a second number uniquely identifies an activity within the session, allowing a session to include a plurality of activities. The identifier may also include a session name and/or a session description. Other information about the video data (e.g., video length, video source, etc.) (i.e., “video metadata”) can also be stored and linked to the video data. Biometric data is preferably linked to at least the start time (e.g., the same start time linked to the video data), the identifier (e.g., the same identifier linked to the video data), and a sample rate, which identifies the rate at which biometric data is received and/or stored.
Once the video and biometric data is stored and linked, algorithms can be used to display the data together. For example, if biometric data is stored at a sample rate of 30 samples per minute (spm), algorithms can be used to display a first biometric value (e.g., below the video data, superimposed over the video data, etc.) at the start of the video clip, a second biometric value two seconds later (two seconds into the video clip), a third biometric value two seconds later (four seconds into the video clip), etc. In alternate embodiments of the present invention, non-video data (e.g., biometric data, self-realization data, etc.) can be stored with a plurality of time-stamps (e.g., individual stamps or offsets for each stored value, or individual sample rates for each data type), which can be used together with the start time to synchronize non-video data to video data.
In one embodiment of the present invention, the biometric device may include a sensor for sensing biometric data, a display for interfacing with the user and displaying various information (e.g., biometric data, set-up data, operation data, such as start, stop, and pause, etc.), a memory for storing the sensed biometric data, a transceiver for communicating with the exemplary computing device, and a processor for operating and/or driving the transceiver, memory, sensor, and display. The exemplary computing device includes a transceiver (1) for receiving biometric data from the exemplary biometric device, a memory for storing the biometric data, a display for interfacing with the user and displaying various information (e.g., biometric data, set-up data, operation data, such as start, stop, and pause, input in-session comments or add voice notes, etc.), a keyboard (or other user input) for receiving user input data, a transceiver (2) for providing the biometric data to the host computing device via the Internet, and a processor for operating and/or driving the transceiver (1), transceiver (2), keyboard, display, and memory.
The keyboard (or other input device) in the computing device, or alternatively the keyboard (or other input device) in the biometric device, may be used to enter self-realization data, or data on how the user is feeling at a particular time. For example, if the user is feeling tired, the user may enter the “T” on the keyboard. If the user is feeling their endorphins kick in, the user may enter the “E” on the keyboard. And if the user is getting their second wind, the user may enter the “S” on the keyboard. Alternatively, to further facilitate operation during the exercise, or sporting activity, short-code key buttons such as “T,” “E,” and “S” can be preassigned, like speed-dial telephone numbers for frequently called contacts on a smart phone, etc., which can be selected manually or using voice recognition. This data (e.g., the entry or its representation) is then stored and linked to either a sample rate (like biometric data) or time-stamp data, which may be a time or an offset to the start time that each button was pressed. This would allow the self-realization data to be synchronized to the video data. It would also allow the self-realization data, like biometric data, to be searched or filtered (e.g., in order to find video corresponding to a particular event, such as when the user started to feel tired, etc.).
In an alternate embodiment of the present invention, the computing device (e.g., a smart phone, etc.) is also in communication with a host computing device via a wide area network (“WAN”), such as the Internet. This embodiment allows the computing device to download the application from the host computing device, offload at least some of the above-identified functions to the host computing device, and store data on the host computing device (e.g., allowing video data, alone or synchronized to non-video data, such as biometric data and self-realization data, to be viewed by another networked device). For example, the software operating on the computing device (e.g., the application, program, etc.) may allow the user to play the video and/or audio data, but not to synchronize the video and/or audio data to the biometric data. This may be because the host computing device is used to store data critical to synchronization (time-stamp index, metadata, biometric data, sample rate, etc.) and/or software operating on the host computing device is necessary for synchronization. By way of another example, the software operating on the computing device may allow the user to play the video and/or audio data, either alone or synchronized with the biometric data, but may not allow the computing device (or may limit the computing device’s ability) to search or otherwise extrapolate from, or process the biometric data to identify relevant portions (e.g., which may be used to create a “highlight reel” of the synchronized video/audio/biometric data) or to rank the biometric and/or video data. This may be because the host computing device is used to store data critical to search and/or to rank the biometric data (biometric data, biometric metadata, etc.), and/or software necessary for searching (or performing advanced searching of) and/or ranking (or performing advanced ranking of) the biometric data.
In one embodiment of the present invention, the video data, which may also include audio data, starts at a time “T” and continues for a duration of “n.” The video data is preferably stored in memory (locally and/or remotely) and linked to other data, such as an identifier, start time, and duration. Such data ties the video data to at least a particular session, a particular start time, and identifies the duration of the video included therein. In one embodiment of the present invention, each session can include different activities. For example, a trip to Berlin on a particular day (session) may involve a bike ride through the city (first activity) and a walk through a park (second activity). Thus, the identifier may include both a session identifier, uniquely identifying the session via a globally unique identifier (GUID), and an activity identifier, uniquely identifying the activity via a globally unique identifier (GUID), where the session/activity relationship is that of a parent/child.
In one embodiment of the present invention, the biometric data is stored in memory and linked to the identifier and a sample rate “m.” This allows the biometric data to be linked to video data upon playback. For example, if identifier is one, start time is 1:00 PM, video duration is one minute, and the sample rate is 30 spm, then the playing of the video at 2:00 PM would result in the first biometric value to be displayed (e.g., below the video, over the video, etc.) at 2:00 PM, the second biometric value to be displayed (e.g., below the video, over the video, etc.) two seconds later, and so on until the video ends at 2:01 PM. While self-realization data can be stored like biometric data (e.g., linked to a sample rate), if such data is only received periodically, it may be more advantageous to store this data linked to the identifier and a time-stamp, where “m” is either the time that the self-realization data was received or an offset between this time and the start time (e.g., ten minutes and four seconds after the start time, etc.). By storing video and non-video data separately from one another, data can be easily search and synchronized.
With respect to linking data to an identifier, which may be linked to other data (e.g., start time, sample rate, etc.), if the data is received in real-time, the data can be linked to the identifier (s) for the current session (and/or activity). However, when data is received after the fact (e.g., after a session has ended), there are several ways in which the data can be linked to a particular session and/or activity (or identifier (s) associated therewith). The data can be manually linked (e.g., by the user) or automatically linked via the application. With respect to the latter, this can be accomplished, for example, by comparing the duration of the received data (e.g., the video length) with the duration of the session and/or activity, by assuming that the received data is related to the most recent session and/or activity, or by analyzing data included within the received data. For example, in one embodiment, data included with the received data (e.g., metadata) may identify a time and/or location associated with the data, which can then be used to link the received data to the session and/or activity. In another embodiment, the computing device could display data (e.g., a barcode, such as a QR code, etc.) that identifies the session and/or activity. An external video recorder could record the identifying data (as displayed by the computing device) along with (e.g., before, after, or during) the user and/or his/her surroundings. The application could then search the video data for identifying data, and use this data to link the video data to a session and/or activity. The identifying portion of the video data could then be deleted by the application if desired.
A more complete understanding of a system and method for using, processing, and displaying biometric data, or a resultant thereof, will be afforded to those skilled in the art, as well as a realization of additional advantages and objects thereof, by a consideration of the following detailed description of the preferred embodiment. Reference will be made to the appended sheets of drawings, which will first be described briefly.
BRIEF DESCRIPTION OF THE DRAWINGS
FIG. 1 illustrates a system for using, processing, and displaying biometric data, and for synchronizing biometric data with other data (e.g., video data, audio data, etc.) in accordance with one embodiment of the present invention;
FIG. 2A illustrates a system for using, processing, and displaying biometric data, and for synchronizing biometric data with other data (e.g., video data, audio data, etc.) in accordance with another embodiment of the present invention;
FIG. 2B illustrates a system for using, processing, and displaying biometric data, and for synchronizing biometric data with other data (e.g., video data, audio data, etc.) in accordance with yet another embodiment of the present invention;
FIG. 3 illustrates an exemplary display of video data synchronized with biometric data in accordance with one embodiment of the present invention;
FIG. 4 illustrates a block diagram for using, processing, and displaying biometric data, and for synchronizing biometric data with other data (e.g., video data, audio data, etc.) in accordance with one embodiment of the present invention;
FIG. 5 illustrates a block diagram for using, processing, and displaying biometric data, and for synchronizing biometric data with other data (e.g., video data, audio data, etc.) in accordance with another embodiment of the present invention;
FIG. 6 illustrates a method for synchronizing video data with biometric data, operating the video data, and searching the biometric data, in accordance with one embodiment of the present invention;
FIG. 7 illustrates an exemplary display of video data synchronized with biometric data in accordance with another embodiment of the present invention;
FIG. 8 illustrates exemplary video data, which is preferably linked to an identifier (ID), a start time (T), and a finish time or duration (n);
FIG. 9 illustrates an exemplary identifier (ID), comprising a session identifier and an activity identifier;
FIG. 10 illustrates exemplary biometric data, which is preferably linked to an identifier (ID), a start time (T), and a sample rate (S);
FIG. 11 illustrates exemplary self-realization data, which is preferably linked to an identifier (ID) and a time (m);
FIG. 12 illustrates how sampled biometric data points can be used to extrapolate other biometric data point in accordance with one embodiment of the present invention;
FIG. 13 illustrates how sampled biometric data points can be used to extrapolate other biometric data points in accordance with another embodiment of the present invention;
FIG. 14 illustrates an example of how a start time and data related thereto (e.g., sample rate, etc.) can be used to synchronized biometric data and self-realization data to video data;
FIG. 15 depicts an exemplary “sign in” screen shot for an application that allows a user to capture at least video and biometric data of the user performing an athletic event (e.g., bike riding, etc.) and to display the video data together (or in synchronization) with the biometric data;
FIG. 16 depict an exemplary “create session” screen shot for the application depicted in FIG. 15, allowing the user to create a new session;
FIG. 17 depicts an exemplary “session name” screen shot for the application depicted in FIG. 15, allowing the user to enter a name for the session;
FIG. 18 depicts an exemplary “session description” screen shot for the application depicted in FIG. 15, allowing the user to enter a description for the session;
FIG. 19 depicts an exemplary “session started” screen shot for the application depicted in FIG. 15, showing the video and biometric data received in real-time;
FIG. 20 depicts an exemplary “review session” screen shot for the application depicted in FIG. 15, allowing the user to playback the session at a later time;
FIG. 21 depicts an exemplary “graph display option” screen shot for the application depicted in FIG. 15, allowing the user to select data (e.g., heart rate data, etc.) to be displayed along with the video data;
FIG. 22 depicts an exemplary “review session” screen shot for the application depicted in FIG. 15, where the video data is displayed together (or in synchronization) with the biometric data;
FIG. 23 depicts an exemplary “map” screen shot for the application depicted in FIG. 15, showing GPS data displayed on a Google map;
FIG. 24 depicts an exemplary “summary” screen shot for the application depicted in FIG. 15, showing a summary of the session;
FIG. 25 depicts an exemplary “biometric search” screen shot for the application depicted in FIG. 15, allowing a user to search the biometric data for particular biometric event (e.g., a particular value, a particular range, etc.);
FIG. 26 depicts an exemplary “first result” screen shot for the application depicted in FIG. 15, showing a first result for the biometric event shown in FIG. 25, together with corresponding video;
FIG. 27 depicts an exemplary “second result” screen shot for the application depicted in FIG. 15, showing a second result for the biometric event shown in FIG. 25, together with corresponding video;
FIG. 28 depicts an exemplary “session search” screen shot for the application depicted in FIG. 15, allowing a user to search for sessions that meet certain criteria; and
FIG. 29 depicts an exemplary “list” screen shot for the application depicted in FIG. 15, showing a result for the criteria shown in FIG. 28.
DETAILED DESCRIPTION OF THE PREFERRED EMBODIMENT
The present invention provides a system and method for using, processing, indexing, benchmarking, ranking, comparing and displaying biometric data, or a resultant thereof, either alone or together (e.g., in synchronization) with other data (e.g., video data, etc.). It should be appreciated that while the invention is described herein in terms of certain biometric data (e.g., heart rate, breathing patterns, blood-alcohol level, etc.), the invention is not so limited, and can be used in conjunction with any biometric and/or physical data, including, but not limited to oxygen levels, CO2 levels, oxygen saturation, blood pressure, blood glucose, lung function, eye pressure, body and ambient conditions (temperature, humidity, light levels, altitude, and barometric pressure), speed (walking speed, running speed), location and distance travelled, breathing rate, heart rate variance (HRV), EKG data, perspiration levels, calories consumed and/or burnt, ketones, waste discharge content and/or levels, hormone levels, blood content, saliva content, audible levels (e.g., snoring, etc.), mood levels and changes, galvanic skin response, brain waves and/or activity or other neurological measurements, sleep patterns, physical characteristics (e.g., height, weight, eye color, hair color, iris data, fingerprints, etc.) or responses (e.g., facial changes, iris (or pupal) changes, voice (or tone) changes, etc.), or any combination or resultant thereof.
As shown in FIG. 1, a biometric device 110 may be in communication with a computing device 108, such as a smart phone, which, in turn, is in communication with at least one computing device (102, 104, 106) via a wide area network (“WAN”) 100, such as the Internet. The computing devices can be of different types, such as a PC, laptop, tablet, smart phone, smart watch etc., using one or different operating systems or platforms. In one embodiment of the present invention, the biometric device 110 is configured to acquire (e.g., measure, sense, estimate, etc.) an individual’s heart rate (e.g., biometric data). The biometric data is then provided to the computing device 108, which includes a video and/or audio recorder (not shown).
In a first embodiment of the present invention, the video and/or audio data are provided along with the heart rate data to a host computing device 106 via the network 100. Because the concurrent video and/or audio data and the heart rate data are provided to the host computing device 106, a host application operating thereon (not shown) can be used to synchronize the video data, audio data, and/or heart rate data, thereby allowing a user (e.g., via the user computing devices 102, 104) to view the video data and/or listen to the audio data (either in real-time or time delayed) while viewing the biometric data. For example, as shown in FIG. 3, the host application may use a time-stamp 320, or other sequencing method using metadata, to synchronize the video data 310 with the biometric data 330, allowing a user to view, for example, an individual (e.g., patient in a hospital, baby in a crib, etc.) at a particular time 340 (e.g., 76 seconds past the start time) and biometric data associated with the individual at that particular time 340 (e.g., 76 seconds past the start time).
It should be appreciated that the host application may further be configured to perform other functions, such as search for a particular activity in video data, audio data, biometric data and/or metadata, and/or ranking video data, audio data, and/or biometric data. For example, the host application may allow the user to search for a particular biometric event, such as a heart rate that has exceeded a particular threshold or value, a heart rate that has dropped below a particular threshold or value, a particular heart rate (or range) for a minimum period of time, etc. By way of another example, the host application may rank video data, audio data, biometric data, or a plurality of synchronized clips (e.g., highlight reels) chronologically, by biometric magnitude (highest to lowest, lowest to highest, etc.), by review (best to worst, worst to best, etc.), or by views (most to least, least to most, etc.). It should further be appreciated that such functions as the ranking, searching, and analysis of data is not limited to a user’s individual session, but can be performed across any number of individual sessions of the user, as well as the session or number of sessions of multiple users. One use of this collection of all the various information (video, biometric and other) is to be able to generate sufficient data points for Big Data analysis and Machine Learning of the purposes of generating AI inferences and recommendations.
By way of example, machine learning algorithms could be used to search through video data automatically, looking for the most compelling content which would subsequently be stitched together into a short “highlight reel.” The neural network could be trained using a plurality of sports videos, along with ratings from users of their level of interest as the videos progress. The input nodes to the network could be a sample of change in intensity of pixels between frames along with the median excitement rating of the current frame. The machine learning algorithms could also be used, in conjunction with a multi-layer convolutional neural network, to automatically classify video content (e.g., what sport is in the video). Once the content is identified, either automatically or manually, algorithms can be used to compare the user’s activity to an idealized activity. For example, the system could compare a video recording of the user’s golf swing to that of a professional golfer. The system could then provide incremental tips to the user on how the user could improve their swing. Algorithms could also be used to predict fitness levels for users (e.g., if they maintain their program, giving them an incentive to continue working out), match users to other users or practitioners having similar fitness levels, and/or create routines optimized for each user.
It should also be appreciated, as shown in FIG. 2A, that the biometric data may be provided to the host computing device 106 directly, without going through the computing device 108. For example, the computing device 108 and the biometric device 110 may communicate independently with the host computing device, either directly or via the network 100. It should further be appreciated that the video data, the audio data, and/or the biometric data need not be provided to the host computing device 106 in real-time. For example, video data could be provided at a later time as long as the data can be identified, or tied to a particular session. If the video data can be identified, it can then be synchronized to other data (e.g., biometric data) received in real-time.
In one embodiment of the present invention, as shown in FIG. 2B, the system includes a computing device 200, such as a smart phone, in communication with a plurality of devices, including a host computing device 240 via a WAN (see, e.g., FIG. 1 at 100), third party devices 250 via the WAN (see, e.g., FIG. 1 at 100), and local devices 230 (e.g., via wireless or wired connections). In a preferred embodiment, the computing device 200 downloads a program or application (i.e., client platform) from the host computing device 240 (e.g., company cloud). The client platform includes a plurality of modules that are configured to perform a plurality of functions.
For example, the client platform may include a video capture module 210 for receiving video data from an internal and/or external camera, and a biometric capture module 212 for receiving biometric data from an internal and/or external biometric device. The client platform may also include a user interface module 202, allowing a user to interact with the platform, a video editing module 204 for editing video data, a file handling module 206 for managing (e.g., storing, linking, etc.) data (e.g., video data, biometric data, identification data, start time data, duration data, sample rate data, self-realization data, time-stamp data, etc.), a database and sync module 214 for replicating data (e.g., copying data stored on the computing device 200 to the host computing device 240 and/or copying user data stored on the host computing device 240 to the computing device 200), an algorithm module 216 for processing received data (e.g., synchronizing data, searching/filtering data, creating a highlight reel, etc.), a sharing module 220 for sharing and/or storing data (e.g., video data, highlight reel, etc.) relating either to a single session or multiple sessions, and a central login and ID module 218 for interfacing with third party social media websites, such as Facebook™.
With respect to FIG. 2B, the computing device 200, which may be a smart phone, a tablet, or any other computing device, may be configured to download the client platform from the host computing device 240. Once the client platform is running on the computing device 200, the platform can be used to start a new session, receive video data for the session (i.e., via the video capture module 210) and receive biometric data for the session (i.e., via the biometric capture module 212). This data can be stored in local storage, in a local database, and/or on a remote storage device (e.g., in the company cloud or a third-party cloud, such as Dropbox™, etc.). In a preferred embodiment, the data is stored so that it is linked to information that (i) identifies the session and (ii) enables synchronization.
For example, video data is preferably linked to at least a start time (e.g., a start time of the session) and an identifier. The identifier may be a single number uniquely identifying the session, or a plurality of numbers (e.g., a plurality of globally (or universally) unique identifiers (GUIDs/UUIDs), where a first number uniquely identifying the session and a second number uniquely identifies an activity within the session, allowing a session (e.g., a trip to or an itinerary in a destination, such as Berlin) to include a plurality of activities (e.g., a bike ride, a walk, etc.). By way of example only, an activity (or session) identifier may be a 128 bit identifier that has a high probability of uniqueness, such as 8bf25512-f17a-4e9e-b49a-7c3f59ec1e85). The identifier may also include a session name and/or a session description. Other information about the video data (e.g., video length, video source, etc.) (i.e., “video metadata”) can also be stored and linked to the video data. Biometric data is preferably linked to at least the start time (e.g., the same start time linked to the video data), the identifier (e.g., the same identifier linked to the video data), and a sample rate, which identifies the rate at which biometric data is received and/or stored. For example, heart rate data may be received and stored at a rate of thirty samples per minute (30 spm), i.e., once every two seconds, or some other predetermined time interval sample.
In some cases, the sample rate used by the platform may be the sample rate of the biometric device (i.e., the rate at which data is provided by the biometric device). In other cases, the sample rate used by the platform may be independent from the rate at which data is received (e.g., a fixed rate, a configurable rate, etc.). For example, if the biometric device is configured to provide biometric data at a rate of sixty samples per minute (60 spm), the platform may still store the data at a rate of 30 spm. In other words, with a sample rate of 30 spm, the platform will have stored five values after ten seconds, the first value being the second value transmitted by the biometric device, the second value being the fourth value transmitted by the biometric device, and so on. Alternatively, if the biometric device is configured to provide biometric data only when the biometric data changes, the platform may still store the data at a rate of 30 spm. In this case, the first value stored by the platform may be the first value transmitted by the biometric device, the second value stored may be the first value transmitted by the biometric device if at the time of storage no new value has been transmitted by the biometric device, the third value stored may be the second value transmitted by the biometric device if at the time of storage a new value is being transmitted by the biometric device, and so on.
Once the video and biometric data is stored and linked, algorithms can be used to display the data together. For example, if biometric data is stored at a sample rate of 30 spm, which may be fixed or configurable, algorithms (e.g., 216) can be used to display a first biometric value (e.g., below the video data, superimposed over the video data, etc.) at the start of the video clip, a second biometric value two seconds later (two seconds into the video clip), a third biometric value two seconds later (four seconds into the video clip), etc. In alternate embodiments of the present invention, non-video data (e.g., biometric data, self-realization data, etc.) can be stored with a plurality of time-stamps (e.g., individual stamps or offsets for each stored value), which can be used together with the start time to synchronize non-video data to video data.
It should be appreciated that while the client platform can be configured to function autonomously (i.e., independent of the host network device 240), in one embodiment of the present invention, certain functions of the client platform are performed by the host network device 240, and can only be performed when the computing device 200 is in communication with the host computing device 240. Such an embodiment is advantageous in that it not only offloads certain functions to the host computing device 240, but it ensures that these functions can only be performed by the host computing device 240 (e.g., requiring a user to subscribe to a cloud service in order to perform certain functions). Functions offloaded to the cloud may include functions that are necessary to display non-video data together with video data (e.g., the linking of information to video data, the linking of information to non-video data, synchronizing non-video data to video data, etc.), or may include more advanced functions, such as generating and/or sharing a “highlight reel.” In alternate embodiments, the computing device 200 is configured to perform the foregoing functions as long as certain criteria has been met. This criteria may include the computing device 200 being in communication with the host computing device 240, or the computing device 200 previously being in communication with the host computing device 240 and the period of time since the last communication being equal to or less than a predetermined amount of time. Technology known to those skilled in the art (e.g., using a keyed hash-based method authentication code (HMAC), a stored time of said last communication (allowing said computing device to determine whether said delta is less than a predetermined amount of time), etc.) can be used to ensure that this criteria is met before allowing the performance of certain functions.
Block diagrams of an exemplary computing device and an exemplary biometric device are shown in FIG. 5. In particular, the exemplary biometric device 500 includes a sensor for sensing biometric data, a display for interfacing with the user and displaying various information (e.g., biometric data, set-up data, operation data, such as start, stop, and pause, etc.), a memory for storing the sensed biometric data, a transceiver for communicating with the exemplary computing device 600, and a processor for operating and/or driving the transceiver, memory, sensor, and display. The exemplary computing device 600 includes a transceiver (1) for receiving biometric data from the exemplary biometric device 500 (e.g., using any of telemetry, any WiFi standard, DNLA, Apple AirPlay, Bluetooth, near field communication (NFC), RFID, ZigBee, Z-Wave, Thread, Cellular, a wired connection, infrared or other method of data transmission, datacasting or streaming, etc.), a memory for storing the biometric data, a display for interfacing with the user and displaying various information (e.g., biometric data, set-up data, operation data, such as start, stop, and pause, input in-session comments or add voice notes, etc.), a keyboard for receiving user input data, a transceiver (2) for providing the biometric data to the host computing device via the Internet (e.g., using any of telemetry, any WiFi standard, DNLA, Apple AirPlay, Bluetooth, near field communication (NFC), RFID, ZigBee, Z-Wave, Thread, Cellular, a wired connection, infrared or other method of data transmission, datacasting or streaming, etc.), and a processor for operating and/or driving the transceiver (1), transceiver (2), keyboard, display, and memory.
The keyboard in the computing device 600, or alternatively the keyboard in biometric device 500, may be used to enter self-realization data, or data on how the user is feeling at a particular time. For example, if the user is feeling tired, the user may hit the “T” button on the keyboard. If the user is feeling their endorphins kick in, the user may hit the “E” button on the keyboard. And if the user is getting their second wind, the user may hit the “S” button on the keyboard. This data is then stored and linked to either a sample rate (like biometric data) or time-stamp data, which may be a time or an offset to the start time that each button was pressed. This would allow the self-realization data, in the same way as the biometric data, to be synchronized to the video data. It would also allow the self-realization data, like the biometric data, to be searched or filtered (e.g., in order to find video corresponding to a particular event, such as when the user started to feel tired, etc.).
It should be appreciated that the present invention is not limited to the block diagrams shown in FIG. 5, and a biometric device and/or a computing device that includes fewer or more components is within the spirit and scope of the present invention. For example, a biometric device that does not include a display, or includes a camera and/or microphone is within the spirit and scope of the present invention, as are other data-entry devices or methods beyond a keyboard, such as a touch screen, digital pen, voice/audible recognition device, gesture recognition device, so-called “wearable,” or any other recognition device generally known to those skilled in the art. Similarly, a computing device that only includes one transceiver, further includes a camera (for capturing video) and/or microphone (for capturing audio or for performing spatial analytics through recording or measurement of sound and how it travels), or further includes a sensor (see FIG. 4) is within the spirit and scope of the present invention. It should also be appreciated that self-realization data is not limited to how a user feels, but could also include an event that the user or the application desires to memorialize. For example, the user may want to record (or time-stamp) the user biking past wildlife, or a particular architectural structure, or the application may want to record (or time-stamp) a patient pressing a “request nurse” button, or any other sensed non-biometric activity of the user.
Referring back to FIG. 1, as discussed above in conjunction with FIG. 2B, the host application (or client platform) may operate on the computing device 108. In this embodiment, the computing device 108 (e.g., a smart phone) may be configured to receive biometric data from the biometric device 110 (either in real-time, or at a later stage, with a time-stamp corresponding to the occurrence of the biometric data), and to synchronize the biometric data with the video data and/or the audio data recorded by the computing device 108 (or a camera and/or microphone operating thereon). It should be appreciated that in this embodiment of the present invention, other than the host application being run locally (e.g., on the computing device 108), the host application (or client platform) operates as previously discussed.
Again, with reference to FIG. 1, in another embodiment of the present invention, the computing device 108 further includes a sensor for sensing biometric data. In this embodiment of the present invention, the host application (or client platform) operates as previously discussed (locally on the computing device 108), and functions to at least synchronize the video, audio, and/or biometric data, and allow the synchronized data to be played or presented to a user (e.g., via a display portion, via a display device connected directly to the computing device, via a user computing device connected to the computing device (e.g., directly, via the network, etc.), etc.).
It should be appreciated that the present invention, in any embodiment, is not limited to the computing devices (number or type) shown in FIGS. 1 and 2, and may include any of a computing, sensing, digital recording, GPS or otherwise location-enabled device (for example, using WiFi Positioning Systems “WPS”, or other forms of deriving geographical location, such as through network triangulation), generally known to those skilled in the art, such as a personal computer, a server, a laptop, a tablet, a smart phone, a cellular phone, a smart watch, an activity band, a heart-rate strap, a mattress sensor, a shoe sole sensor, a digital camera, a near field sensor or sensing device, etc. It should also be appreciated that the present invention is not limited to any particular biometric device, and includes biometric devices that are configured to be worn on the wrist (e.g., like a watch), worn on the skin (e.g., like a skin patch) or scalp, or incorporated into computing devices (e.g., smart phones, etc.), either integrated in, or added to items such as bedding, wearable devices such as clothing, footwear, helmets or hats, or ear phones, or athletic equipment such as rackets, golf clubs, or bicycles, where other kinds of data, including physical performance metrics such as racket or club head speed, or pedal rotation/second, or footwear recording such things as impact zones, gait or shear, can also be measured synchronously with biometrics, and synchronized to video. Other data can also be measured synchronously with video data, including biometrics on animals (e.g., a bull’s acceleration or pivot or buck in a bull riding event, a horse’s acceleration matched to heart rate in a horse race, etc.), and physical performance metrics of inanimate objects, such a revolutions/minute (e.g., in a vehicle, such as an automobile, a motorcycle, etc.), miles/hour (or the like) (e.g., in a vehicle, such as an automobile, a motorcycle, etc., a bicycle, etc.), or G-forces (e.g., experienced by the user, an animal, and inanimate object, etc.). All of this data (collectively “non-video data,” which may include metadata, or data on non-video data) can be synchronized to video data using a sample rate and/or at least one time-stamp, as discussed above.
It should further be appreciated that the present invention need not operate in conjunction with a network, such as the Internet. For example, as shown in FIG. 2A, the biometric device 110, which may be, for example, be a wireless activity band for sensing heart rate, and the computing device 108, which may be, for example, a digital video recorder, may be connected directly to the host computing device 106 running the host application (not shown), where the host application functions as previously discussed. In this embodiment, the video, audio, and/or biometric data can be provided to the host application either (i) in real time, or (ii) at a later time, since the data is synchronized with a sample rate and/or time-stamp. This would allow, for example, at least video of an athlete, or a sportsman or woman (e.g., a football player, a soccer player, a racing driver, etc.) to be shown in action (e.g., playing football, playing soccer, motor racing, etc.) along with biometric data of the athlete in action (see, e.g., FIG. 7). By way of example only, this would allow a user to view a soccer player’s heart rate 730 as the soccer player dribbles a ball, kicks the ball, heads the ball, etc. This can be accomplished using a time stamp 720 (e.g., start time, etc.), or other sequencing method using metadata (e.g., sample rate, etc.), to synchronize the video data 710 with the biometric data 730, allowing the user to view the soccer player at a particular time 740 (e.g., 76 seconds) and biometric data associated with the athlete at that particular time 340 (e.g., 76 seconds). Similar technology can be used to display biometric data on other athletes, card players, actors, online garners, etc.
Where it is desirable to monitor or watch more than one individual from a camera view, for example, patients in a hospital ward being observed from a remote nursing station or, during a televised broadcast of a sporting event such as a football game, with multiple players on the sports field, the system can be so configured, by the subjects using Bluetooth or other wearable or NFC sensors (in some cases with their sensing capability also being location-enabled in order to identify which specific individual to track) capable of transmitting their biometrics over practicable distances, in conjunction with relays or beacons if necessary, such that the viewer can switch the selection of which of one or multiple individuals’ biometric data to track, alongside the video or broadcast, and, if wanted and where possible within the limitations of the video capture field of the camera used, also to concentrate the view of the video camera on a reduced group or on a specific individual. In an alternate embodiment of the present invention, selection of biometric data is automatically accomplished, for example, based on the individual’s location in the video frame (e.g., center of the frame), rate of movement (e.g., moving quicker than other individuals), or proximity to a sensor (e.g., being worn by the individual, embedded in the ball being carried by the individual, etc.), which may be previously activate or activated by a remote radio frequency signal. Activation of the sensor may result in biometric data of the individual being transmitted to a receiver, or may allow the receiver to identified biometric data of the individual amongst other data being transmitted (e.g., biometric data from other individuals).
In the context of fitness or sports tracking, it should be appreciated that the capturing of an individual’s activity on video is not dependent on the presence of a third party to do this, but various methods of self-videoing can be envisaged, such as a video capture device mounted on the subject’s wrist or a body harness, or on a selfie attachment or a gimbal, or fixed to an object (e.g., sports equipment such as bicycle handlebars, objects found in sporting environments such as a basketball or tennis net, a football goal post, a ceiling, etc., a drone-borne camera following the individual, a tripod, etc.). It should be further noted that such video capture devices can include more than one camera lens, such that not only the individual’s activity may be videoed, but also simultaneously a different view, such as what the individual is watching or sees in front of them (i.e., the user’s surroundings). The video capture device could also be fitted with a convex mirror lens, or have a convex mirror added as an attachment on the front of the lens, or be a full 360 degree camera, or multiple 360 cameras linked together, such that either with or without the use of specialized software known in the art, a 360 degree all-around or surround view can be generated, or a 360 global view in all axes can be generated.
In the context of augmented or virtual reality, where the individual is wearing suitably equipped augmented reality (“AR”) or virtual reality (“VR”) glasses, goggles, headset or is equipped with another type of viewing display capable of rendering AR, VR, or other synthesized or real 3D imagery, the biometric data such as heart rate from the sensor, together with other data such as, for example, work-out run or speed, from a suitably equipped sensor, such as an accelerometer capable of measuring motion and velocity, could be viewable by the individual, superimposed on their viewing field. Additionally an avatar of the individual in motion could be superimposed in front of the individual’s viewing field, such that they could monitor or improve their exercise performance, or otherwise enhance the experience of the activity by viewing themselves or their own avatar, together (e.g., synchronized) with their performance (e.g., biometric data, etc.). Optionally, the biometric data also of their avatar, or the competing avatar, could be simultaneously displayed in the viewing field. In addition (or alternatively), at least one additional training or competing avatar can be superimposed on the individual’s view, which may show the competing avatar (s) in relation to the individual (e.g., showing them superimposed in front of the individual, showing them superimposed to the side of the user, showing them behind the individual (e.g., in a rear-view-mirror portion of the display, etc.), and/or showing them in relation to the individual (e.g., as blips on a radar-screen portion of the display, etc.), etc. Competing avatar (s), either of real people such as their friends or training acquaintances, can be used to motivate the user to improve or correct their performance and/or to make their exercise routine more interesting (e.g., by allowing the individual to “compete” in the AR, VR, or Mixed Reality (“MR”) environment while exercising, or training, or virtually “gamifying” their activity through the visualization of virtual destinations or locations, imagined or real, such as historical sites, scanned or synthetically created through computer modeling).
Additionally, any multimedia sources to which the user is being exposed whilst engaging in the activity which is being tracked and recorded, should similarly be able to be recorded with the time stamp, for analysis and/or correlation of the individual’s biometric response. An example of an application of this could be in the selection of specific music tracks for when someone is carrying out a training activity, where the correlation of the individual’s past response, based, for example, on heart rate (and how well they achieved specific performance levels or objectives) to music type (e.g., the specific music track (s), a track (s) similar to the specific track (s), a track (s) recommended or selected by others who have listened to or liked the specific track (s), etc.) is used to develop a personalized algorithm, in order to optimize automated music selection to either enhance the physical effort, or to maximize recovery during and after exertion. The individual could further specify that they wished for the specific track or music type, based upon the personalized selection algorithm, to be played based upon their geographical location; an example of this would be someone who frequently or regularly uses a particular circuit for training or recreational purposes. Alternatively, tracks or types of music could be selected through recording or correlation of past biometric response in conjunction with self-realization inputting when particular tracks were being listened to.
It should be appreciated that biometric data does not need to be linked to physical movement or sporting activity, but may instead be combined with video of an individual at a fixed location (e.g., where the individual is being monitored remotely or recorded for subsequent review), for example, as shown in FIG. 3, for health reasons or a medical condition, such as in their home or in hospital, or a senior citizen in an assisted-living environment, or a sleeping infant being monitored by parents whilst in another room or location.
Alternatively, the individual might be driving past or in the proximity of a park or a shopping mall, with their location being recorded, typically by geo-stamping, or additional information being added by geo-tagging, such as the altitude or weather at the specific location, together with what the information or content is, being viewed or interacted with by the individual (e.g., a particular advertisement, a movie trailer, a dating profile, etc.) on the Internet or a smart/enabled television, or on any other networked device incorporating a screen, and their interaction with that information or content, being viewable or recorded by video, in conjunction with their biometric data, with all these sources of data being able to be synchronized for review, by virtue of each of these individual sources being time-stamped or the like (e.g., sampled, etc.). This would allow a third party (e.g., a service provider, an advertiser, a provider of advertisements, a movie production company/promoter, a poster of a dating profile, a dating site, etc.) to acquire for analysis of their response, the biometric data associated with the viewing of certain data by the viewer, where either the viewer or their profile could optionally be identifiable by the third party’s system, or where only the identity of the viewer’s interacting device is known, or can be acquired from the biometric sending party’s GPS, or otherwise location-enabled, device.
For example, an advertiser or an advertisement provider could see how people are responding to an advertisement, or a movie production company/promoter could evaluate how people are responding to a movie trailer, or a poster of a dating profile or the dating site itself, could see how people are responding to the dating profile. Alternatively, viewers of online players of an online gaming or eSports broadcast service such as twitch.tv, or of a televised or streamed online poker game, could view the active participants’ biometric data simultaneously with the primary video source as well as the participants’ visible reactions or performance. As with video/audio, this can either be synchronized in real-time, or synchronized later using the embedded time-stamp or the like (e.g., sample rate, etc.). Additionally, where facial expression analysis is being generated from the source video, for example in the context of measuring an individual’s response to advertising messages, since the video is already time-stamped (e.g., with a start time), the facial expression data can be synchronized and correlated to the physical biometric data of the individual, which has similarly been time-stamped and/or sampled,
As previously discussed, the host application may be configured to perform a plurality of functions. For example, the host application may be configured to synchronize video and/or audio data with biometric data. This would allow, for example, an individual watching a sporting event (e.g., on a TV, computer screen, etc.) to watch how each player’s biometric data changes during play of the sporting event, or also to map those biometric data changes to other players or other comparison models. Similarly, a doctor, nurse, or medical technician could record a person’s sleep habits, and watch, search or later review, the recording (e.g., on a TV, computer screen, etc.) while monitoring the person’s biometric data. The system could also use machine learning to build a profile for each patient, identifying certain characteristics of the patient (e.g., their heart rate rhythm, their breathing pattern, etc.) and notify a doctor, a nurse, or medical technician or trigger an alarm if the measured characteristics appear abnormal or irregular.
The host application could also be configured to provide biometric data to a remote user via a network, such as the Internet. For example, a biometric device (e.g., a smart phone with a blood-alcohol sensor) could be used to measure a person’s blood-alcohol level (e.g., while the person is talking to the remote user via the smart phone), and to provide the person’s blood-alcohol level to the remote user. By placing the sensor near, or incorporating it in the microphone, such a system would allow a parent to determine whether their child has been drinking alcohol by participating in a telephone or video call with their child. Different sensors known in the art could be used to sense different chemicals in the person’s breath, or detect people’s breathing patterns through analysis of sound and speed variations, allowing the monitoring party to determine whether the subject has been using alcohol or other controlled substances or to conduct breath analysis for other diagnostic reasons.
The system could also be adapted with a so-called “lab on a chip” (LOC) integrated in the device itself, or with a suitable attachment added to it, for the remote testing for example, of blood samples where the smart-phone is either used for the collection and sending of the sample to a testing laboratory for analysis, or is used to carry out the sample collection and analysis within the device itself. In either case the system is adapted such that the identity of the subject and their blood sample are cross-authenticated for the purposes of sample and analysis integrity as well as patient identity certainty, through the simultaneous recording of the time-stamped video and time and/or location (or GPS) stamping of the sample at the point of collection and/or submission of the sample. This confirmation of identity is particularly important for regulatory, record keeping and health insurance reasons in the context of telemedicine, since the individual will increasingly be performing functions which, till now, have been carried out typically on-site at the relevant facility, by qualified and regulated medical or laboratory staff, rather than by the subject using a networked device, either for upload to the central analysis facility, or for remote analysis on the device itself.
This, or the collection of other biometric data such as heart rate or blood pressure, could also be applied in situations where it is critical for safety reasons, to check, via regular remote video monitoring in real time, whether say a pilot of a plane, a truck or train driver, are in fit and sound condition to be in control of their vehicle or vessel or whether for example they are experiencing a sudden incapacity or heart attack etc. Because the monitored person is being videoed at the same time as providing time-stamped, geo-stamped and/or sampled biometric data, there is less possibility for the monitored person or a third party, to “trick”, “spoof” or bypass the system. In a patient/doctor remote consultation setting, the system could be used for secure video consults where also, from a regulatory or health insurance perspective, the consultation and its occurrence is validated through the time and/or geo stamp validation. Furthermore, where there is a requirement for a higher level of authentication, the system could further be adapted to use facial recognition or biometric algorithms, to ensure that the correct person is being monitored, or facial expression analysis could be used for behavioral pattern assessment.
The concern that a monitored party would not wish to be permanently monitored (e.g., a senior citizen not wanting to have their every move and action continuously videoed) could be mitigated by the incorporation of various additional features. In one embodiment, the video would be permanently recording in a loop system which uses a reserved memory space, recording for a predetermined time period, and then, automatically erasing the video, where n represents the selected minutes in the loop and E is the event which prevents the recorded loop of n minutes being erased, and triggers both the real time transmission of the visible state or actions of the monitored person to the monitoring party, as well as the ability to rewind, in order for the monitoring party to be able to review the physical manifestation leading up to E. The trigger mechanism for E could be, for example, the occurrence of biometric data outside the predefined range, or the notification of another anomaly such as a fall alert, activated by movement or location sensors such as a gyroscope, accelerometer or magnetometer within the health band device worn by, say the senior citizen, or on their mobile phone or other networked motion-sensing device in their proximity. The monitoring party would be able not only to view the physical state of the monitored party after E, whilst getting a simultaneous read-out of their relevant biometric data, but also to review the events and biometric data immediately leading up to the event trigger notification. Alternatively, it could be further calibrated so that although video is recorded, as before, in the n loop, no video from the n loop will actually be transmitted to a monitoring party until the occurrence of E. The advantages of this system include the respect of the privacy of the individual, where only the critical event and the time preceding the event would be available to a third party, resulting also in a desired optimization of both the necessary transmission bandwidth and the data storage requirements. It should be appreciated that the foregoing system could also be configured such that the E notification for remote senior, infant or patient monitoring is further adapted to include facial tracking and/or expression recognition features.
Privacy could be further improved for the user if their video data and biometric data are stored by themselves, on their own device, or on their own external, or own secure third-party “cloud” storage, but with the index metadata of the source material, which enables the sequencing, extrapolation, searching and general processing of the source data, remaining at a central server, such as, in the case of medical records for example, at a doctor’s office or other healthcare facility. Such a system would enable the monitoring party to have access to the video and other data at the time of consultation, but with the video etc. remaining in the possession of the subject. A further advantage of separating the hosting of the storage of the video and biometric source data from the treatment of the data, beyond enhancing the user’s privacy and their data security, is that by virtue of its storage locally with the subject, not having to upload it to the computational server results both in reduced cost and increased efficiency of storage and data bandwidth. This would be of benefit also where such kind of remote upload of tests for review by qualified medical staff at a different location from the subject are occurring in areas of lower-bandwidth network coverage. A choice can also be made to lower the frame rate of the video material, provided that this is made consistent with sampling rate to confirm the correct time stamp, as previously described.
It should be appreciated that with information being stored at the central server (or the host device), various techniques known in the art can be implemented to secure the information, and prevent unauthorized individuals or entities from accessing the information. Thus, for example, a user may be provided (or allowed to create) a user name, password, and/or any other identifying (or authenticating) information (e.g., a user biometric, a key fob, etc.), and the host device may be configured to use the identifying (or authenticating) information to grant access to the information (or a portion thereof). Similar security procedures can be implemented for third parties, such as medical providers, insurance companies, etc., to ensure that the information is only accessible by authorized individuals or entities. In certain embodiments, the authentication may allow access to all the stored data, or to only a portion of the stored data (e.g., a user authentication may allow access to personal information as well as stored video and/or biometric data, whereas a third party authentication may only allow access to stored video and/or biometric data). In other embodiments, the authentication is used to determine what services are available to an individual or entity logging into the host device, or the website. For example, visitors to the website (or non-subscribers) may only be able to synchronize video/audio data to biometric data and/or perform rudimentary searching or other processing, whereas a subscriber may be able to synchronize video/audio data to biometric data and/or perform more detailed searching or other processing (e.g., to create a highlight reel, etc.).
It should further be appreciated that while there are advantages to keeping just the index metadata at the central server in the interests of storage and data upload efficiency as well as so providing a common platform for the interoperability of the different data types and storing the video and/or audio data on the user’s own device (e.g., iCloud™, DropBox™, OneDrive™, etc.), the present invention is not so limited. Thus, in certain embodiments, where feasible, it may be beneficial to (1) store data (e.g., video, audio, biometric data, and metadata) on the user’s device (e.g., allowing the user device to operate independent of the host device), (2) store data (e.g., video, audio, biometric data, and metadata) on the central server (e.g., host device) (e.g., allowing the user to access the data from any network-enabled device), or (3) store a first portion (e.g., video and audio data) on the user’s device and store a second portion (e.g., biometric data and metadata) on the central server (e.g., host device) (e.g., allowing the user to only view the synchronized video/audio/biometric data when the user device is in communication with the host device, allowing the user to only search the biometric data (e.g., to create a “highlight reel”) or rank the biometric data (to identify and/or list data chronologically, magnitude (highest to lowest), magnitude (lowest to highest), best reviewed, worst reviewed, most viewed, least viewed, etc.) when the user device is in communication with the host device, etc.).
In another embodiment of the present invention, the functionality of the system is further (or alternatively) limited by the software operating on the user device and/or the host device. For example, the software operating on the user device may allow the user to play the video and/or audio data, but not to synchronize the video and/or audio data to the biometric data. This may be because the central server is used to store data critical to synchronization (time-stamp index, metadata, biometric data, sample rate, etc.) and/or software operating on the host device is necessary for synchronization. By way of another example, the software operating on the user device may allow the user to play the video and/or audio data, either alone or synchronized with the biometric data, but may not allow the user device (or may limit the user device’s ability) to search or otherwise extrapolate from, or process the biometric data to identify relevant portions (e.g., which may be used to create a “highlight reel” of the synchronized video/audio/biometric data) or to rank the biometric and/or video data. This may be because the central server is used to store data critical to search and/or rank the biometric data (biometric data, biometric metadata, etc.), and/or software necessary for searching (or performing advanced searching of) and/or ranking (or performing advanced ranking of) the biometric data.
In any or all of the above embodiments, the system could be further adapted to include password or other forms of authentication to enable secured access (or deny unauthorized access) to the data in either of one or both directions, such that the user requires permission to access the host, or the host to access the user’s data. Where interaction between the user and the monitoring party or host is occurring in real time such as in a secure video consult between patient and their medical practitioner or other medical staff, data could be exchanged and viewed through the establishment of a Virtual Private Network (VPN). The actual data (biometric, video, metadata index, etc.) can alternatively or further be encrypted both at the data source, for example at the individual’s storage, whether local or cloud-based, and/or at the monitoring reviewing party, for example at patient records at the medical facility, or at the host administration level.
In the context of very young infant monitoring, a critical and often unexplained problem is Sudden Infant Death Syndrome (SIDS). Whilst the incidences of SIDS are often unexplained, various devices attempt to prevent its occurrence. However, by combining the elements of the current system to include sensor devices in or near the baby’s crib to measure relevant biometric data including heart rate, sleep pattern, breath analyzer, and other measures such as ambient temperature, together with a recording device to capture movement, audible breathing, or lack thereof (i.e., silence) over a predefined period of time, the various parameters could be set in conjunction with the time-stamped video record, by the parent or other monitoring party, to provide a more comprehensive alert, to initiate a more timely action or intervention by the user, or indeed to decide that no action response would in fact be necessary. Additionally, in the case, for example, of a crib monitoring situation, the system could be so configured to develop from previous observation, with or without input from a monitoring party, a learning algorithm to help in discerning what is “normal,” what is false positive, or what might constitute an anomaly, and therefore a call to action.
The host application could also be configured to play video data that has been synchronized to biometric data, or search for the existence of certain biometric data. For example, as previously discussed, by video recording with sound a person sleeping, and synchronizing the recording with biometric data (e.g., sleep patterns, brain activity, snoring, breathing patterns, etc.), the biometric data can be searched to identify where certain measures such as sound levels, as measured for example in decibels, or periods of silences, exceed or drop below a threshold value, allowing the doctor, nurse, or medical technician to view the corresponding video portion without having to watch the entire video of the person sleeping.
Such a method is shown in FIG. 6, starting at step 700, where biometric data and time stamp data (e.g., start time, sample rate) is received (or linked) at step 702. Audio/video data and time stamp data (e.g., start time, etc.) is then received (or linked) at step 704. The time stamp data (from steps 702 and 704) is then used to synchronize the biometric data with the audio/video data. The user is then allowed to operate the audio/video at step 708. If the user selects play, then the audio/video is played at step 710. If the user selects search, then the user is allowed to search the biometric data at step 712. Finally, if the user selects stop, then the video is stopped at step 714.
It should be appreciated that the present invention is not limited to the steps shown in FIG. 6. For example, a method that allows a user to search for biometric data that meets at least one condition, play the corresponding portion of the video (or a portion just before the condition), and stop the video from playing after the biometric data no longer meets the at least one condition (or just after the biometric data non longer meets the condition) is within the spirit and scope of the present invention. By way of another example, if the method involves interacting between the user device and the host device to synchronize the video/audio data and the biometric data and/or search the biometric data, then the method may further involve the steps of uploading the biometric data and/or metadata to the host device (e.g., in this embodiment the video/audio data may be stored on the user device), and using the biometric data and/or metadata to create a time-stamp index for synchronization and/or to search the biometric data for relevant or meaningful data (e.g., data that exceeds a threshold, etc.). By way of yet another example, the method may not require step 706 if the audio/video data and the biometric data are played together (synchronized) in real-time, or at the time the data is being played (e.g., at step 710).
In one embodiment of the present invention, as shown in FIG. 8, the video data 800, which may also include audio data, starts at a time “T” and continues for a duration of “n.” The video data is preferably stored in memory (locally and/or remotely) and linked to other data, such as an identifier 802, start time 804, and duration 806. Such data ties the video data to at least a particular session, a particular start time, and identifies the duration of the video included therein. In one embodiment of the present invention, each session can include different activities. For example, a trip to a destination in Berlin, or following a specific itinerary on a particular day (session) may involve a bike ride through the city (first activity) and a walk through a park (second activity). Thus, as shown in FIG. 9, the identifier 802 may include both a session identifier 902, uniquely identifying the session via a globally unique identifier (GUID), and an activity identifier 904, uniquely identifying the activity via a globally unique identifier (GUID), where the session/activity relationship is that of a parent/child.
In one embodiment of the present invention, as shown in FIG. 10, the biometric data 1000 is stored in memory and linked to the identifier 802 and a sample rate “m” 1104. This allows the biometric data to be linked to video data upon playback. For example, if identifier 802 is one, start time 804 is 1:00 PM, video duration is one minute, and the sample rate 1104 is 30 spm, then the playing of the video at 2:00 PM would result in the first biometric value (biometric (1)) to be displayed (e.g., below the video, over the video, etc.) at 2:00 PM, the second biometric value (biometric (2)) to be displayed (e.g., below the video, over the video, etc.) two seconds later, and so on until the video ends at 2:01 PM. While self-realization data can be stored like biometric data (e.g., linked to a sample rate), if such data is only received periodically, it may be more advantageous to store this data 110 as shown in FIG. 11, i.e., linked to the identifier 802 and a time-stamp 1104, where “m” is either the time that the self-realization data 1100 was received or an offset between this time and the start time 804 (e.g., ten minutes and four seconds after the start time, etc.).
This can be seen, for example, in FIG. 14, where video data starts at time T, biometric data is sampled every two seconds (30 spm), and self-realization data is received at time T+3 (or three units past the start time). While the video 1402 is playing, a first biometric value 1404 is displayed at time T+1, first self-realization data 1406 is displayed at time T+2, and a second biometric value 1406 is displayed at time T+4. By storing data in this fashion, both video and non-video data can be stored separately from one another and synchronized in real-time, or at the time the video is being played. It should be appreciated that while separate storage of data may be advantageous for devices having minimal memory and/or processing power, the client platform may be configured to create new video data, or data that includes both video and non-video data displayed synchronously. Such a feature may advantageous in creating a highlight reel, which can then be shared using social media websites, such as Facebook™ or Youtube™, and played using standard playback software, such as Quicktime™. As discussed in greater detail below, a highlight reel may include various portions (or clips) of video data (e.g., when certain activity takes place, etc.) along with corresponding biometric data.
When sampled data is subsequently displayed, the client platform can be configured to display this data using certain extrapolation techniques. For example, in one embodiment of the present invention, as shown in FIG. 12, where a first biometric value 1202 is displayed at T+1, a second biometric value 1204 is displayed at T+2, and a third biometric value 1206 is displayed at T+3, biometric data can be displayed at non-sampled times using known extrapolation techniques, including linear and non-linear interpolation and all other extrapolation and/or interpolation techniques generally known to those skilled in the art. In another embodiment of the present invention, as shown in FIG. 13, the first biometric value 1202 remains on the display until the second biometric value 1204 is displayed, the second biometric value 1204 remains on the display until the third biometric value 1206 is displayed, and so on.
With respect to linking data to an identifier, which may be linked to other data (e.g., start time, sample rate, etc.), if the data is received in real-time, the data can be linked to the identifier (s) for the current session (and/or activity). However, when data is received after the fact (e.g., after a session has ended), there are several ways in which the data can be linked to a particular session and/or activity (or identifier (s) associated therewith). The data can be manually linked (e.g., by the user) or automatically linked via the application. With respect to the latter, this can be accomplished, for example, by comparing the duration of the received data (e.g., the video length) with the duration of the session and/or activity, by assuming that the received data is related to the most recent session and/or activity, or by analyzing data included within the received data. For example, in one embodiment, data included with the received data (e.g., metadata) may identify a time and/or location associated with the data, which can then be used to link the received data to the session and/or activity. In another embodiment, the computing device could display or play data (e.g., a barcode, such as a QR code, a sound, such as a repeating sequence of notes, etc.) that identifies the session and/or activity. An external video/audio recorder could record the identifying data (as displayed or played by the computing device) along with (e.g., before, after, or during) the user and/or his/her surroundings. The application could then search the video/audio data for identifying data, and use this data to link the video/audio data to a session and/or activity. The identifying portion of the video/audio data could then be deleted by the application if desired. In an alternate embodiment, a barcode (e.g., a QR code) could be printed on a physical device (e.g., a medical testing module, which may allow communication of medical data over a network (e.g., via a smart phone)) and used (as previously described) to synchronize video of the user using the device to data provided by the device. In the case of a medical testing module, the barcode printed on the module could be used to synchronize video of the testing to the test result provided by the module. In yet another embodiment, both the computing device and the external video/audio recorder are used to record video and/or audio of the user (e.g., the user stating “begin Berlin biking session,” etc.) and to use the user-provided data to link the video/audio data to a session and/or activity. For example, the computing device may be configured to link the user-provided data with a particular session and/or activity (e.g., one that is started, one that is about to start, one that just ended, etc.), and to use the user-provided data in the video/audio data to link the video/audio data to the particular session and/or activity.
In one embodiment of the present invention, the client platform (or application) is configured to operate on a smart phone or a tablet. The platform (either alone or together with software operating on the host device) may be configured to create a session, receive video and non-video data during the session, and playback video data together (synchronized) with non-video data. The platform may also allow a user to search for a session, search for certain video and/or non-video events, and/or create a highlight reel. FIGS. 15-29 show exemplary screen shots of such a platform.
For example, FIG. 15 shows an exemplary “sign in” screen 1500, allowing a user to sign into the application and have access to application-related, user-specific data, as stored on the computing device and/or the host computing device. The login may involve a user ID and password unique to the application, the company cloud, or a social service website, such as Facebook™.
Once the user is signed in, the user may be allowed to create a session via an exemplary “create session” screen 1600, as shown in FIG. 16. In creating a session, the user may be allowed to select a camera (e.g., internal to the computing device, external to the computing device (e.g., accessible via the Internet, connected to the computing device via a wired or wireless connection), etc.) that will be providing video data. Once a camera is selected, video data 1602 from the camera may be displayed on the screen. The user may also be allowed to select a biometric device (e.g., internal to the computing device, external to the computing device (e.g., accessible via the Internet, connected to the computing device via a wired or wireless connection), etc.) that will be providing biometric data. Once a biometric device is selected, biometric data 1604 from the biometric device may be displayed on the screen. The user can then start the session by clicking the “start session” button 1608. While the selection process is preferably performed before the session is started, the user may defer selection of the camera and/or biometric device until after the session is over. This allows the application to receive data that is not available in real-time, or is being provided by a device that is not yet connected to the computing device (e.g., an external camera that will be plugged into the computing device once the session is over).
It should be appreciated that in a preferred embodiment of the present invention, clicking the “start session” button 1608 not only starts a timer 1606 that indicates a current length of the session, but it triggers a start time that is stored in memory and linked to a globally unique identifier (GUID) for the session. By linking the video and biometric data to the GUID, and linking the GUID to the start time, the video and biometric data is also (by definition) linked to the start time. Other data, such as sample rate, can also be linked to the biometric data, either by linking the data to the biometric data, or linking the data to the GUID, which is in turn linked to the biometric data.
Either before the session is started, or after the session is over, the user may be allowed to enter a session name via an exemplary “session name” screen 1700, as shown in FIG. 17. Similarly, the user may also be allowed to enter a session description via an exemplary “session description” screen 1800, as shown in FIG. 18.
FIG. 19 shows an exemplary “session started” screen 1900, which is a screen that the user might see while the session is running. On this screen, the user may see the video data 1902 (if provided in real-time), the biometric data 1904 (if provided in real-time), and the current running time of the session 1906. If the user wishes to pause the session, the user can press the “pause session” button 1908, or if the user wishes to stop the session, the user can press the “stop session” button (not shown). By pressing the “stop session” button (not shown), the session is ended, and a stop time is stored in memory and linked to the session GUID. Alternatively, by pressing the “pause session” button 1908, a pause time (first pause time) is stored in memory and linked to the session GUID. Once paused, the session can then be resumed (e.g., by pressing the “resume session” button, not shown), which will result in a resume time (first resume time) to be stored in memory and linked to the session GUID. Regardless of whether a session is started and stopped (i.e., resulting in a single continuous video), or started, paused (any number of times), resumed (any number of times), and stopped (i.e., resulting in a plurality of video clips), for each start/pause time stored in memory, there should be a corresponding stop/resume time stored in memory.
Once a session has been stopped, it can be reviewed via an exemplary “review session” screen 2000, as shown in FIG. 20. In its simplest form, the review screen may playback video data linked to the session (e.g., either a single continuous video if the session does not include at least one pause/resume, multiple video clips played one after another if the session includes at least one pause/resume, or multiple video clips played together if the multiple video clips are related to one another (e.g., two videos (e.g., from different vantage points) of the user performing a particular activity, a first video of the user performing a particular activity while viewing a second video, such as a training video). If the user wants to see non-video data displayed along with the video data, the user can press the “show graph options” button 2022. By pressing this button, the user is presented with an exemplary “graph display option” screen 2100, as shown in FIG. 21. Here, the user can select data that he/she would like to see along with the video data, such as biometric data (e.g., heart rate, heart rate variance, user speed, etc.), environmental data (e.g., temperature, altitude, GPS, etc.), or self-realization data (e.g., how the user felt during the session). FIG. 22 shows an exemplary “review session” screen 2000 that includes both video data 2202 and biometric data, which may be shown in graph form 2204 or written form 2206. If more than one individual can be seen in the video, the application may be configured to show biometric data on each individual, either at one time, or as selected by the user (e.g., allowing the user to view biometric data on a first individual by selecting the first individual, allowing the user to view biometric data on a second individual by selecting the second individual, etc.).
FIG. 23 shows an exemplary “map” screen 2300, which may be used to show GPS data to the user. Alternatively, GPS data can be presented together with the video data (e.g., below the video data, over the video data, etc.). An exemplary “summary” screen 2400 of the session may also be presented to the user (see FIG. 24), displaying session information such as session name, session description, various metrics, etc.
By storing video and non-video data separately, the data can easily be searched. For example, FIG. 25 shows an exemplary “biometric search” screen 2500, where a user can search for a particular biometric value or range (i.e., a biometric event). By way of example, the user may want to jump to a point in the session where their heart rate is between 95 and 105 beats-per-minute (bpm). FIG. 26 shows an exemplary “first result” screen 2600 where the user’s heart rate is at 100.46 bmp twenty minutes and forty-two seconds into the session (see, e.g., 2608). FIG. 27 shows an exemplary “second result” screen 2700 where the user’s heart rate is at 100.48 bmp twenty-three minutes and forty-eight seconds into the session (see, e.g., 2708). It should be appreciated that other events can be searched for in a session, including video events and self-realization events.
Not only can data within a session be searched, but so too can data from multiple sessions. For example, FIG. 28 shows an exemplary “session search” screen 2800, where a user can enter particular search criteria, including session date, session length, biometric events, video event, self-realization event, etc. FIG. 29 shows an exemplary “list” screen 2900, showing sessions that meet the entered criteria.
The foregoing description of a system and method for using, processing, and displaying biometric data, or a resultant thereof, has been presented for the purposes of illustration and description. It is not intended to be exhaustive or to limit the invention to the precise forms disclosed, and many modifications and variations are possible in light of the above teachings. Those skilled in the art will appreciate that there are a number of ways to implement the foregoing features, and that the present invention it not limited to any particular way of implementing these features. The invention is solely defined by the following claims.
So you can give someone Rona just by sneazing less than six feet away. but they can’t test for it unless they stab your brains out with their swabs, right? We launched this discussion a few months ago, but it hardly caught any attention being heavily censored by fact-fakers and in competition with Gates and Fauci’s 24/7 media circus. Luckily, recent mainstream news have have just revived the topic, and this is essential knowledge for our health and even survival.
A Covid-19 Nasal Swab Test Punctured Woman’s Brain Lining and Leaked Brain Fluid From Her Nose. What does that mean?
ACovid-19 nasal swab test punctured a US woman’s brain lining, causing fluid to leak from her nose and putting her at risk of life-threatening infection, doctors reported in a medical journal Thursday.
The patient, who is in her 40s, had an undiagnosed rare condition and the test she received may have been carried out improperly, a sequence of improbable events that means the risk from nasal tests remains very low.
But her case showed health care professionals should take care to follow testing protocols closely, Jarrett Walsh, senior author of the paper that appeared in JAMA Otolaryngology–Head & Neck Surgery, told AFP.
People who’ve had extensive sinus or skull base surgery should consider requesting oral testing if available, he added.
“It underscores the necessity of adequate training of those performing the test and the need for vigilance after the test has been performed,” added ear, nose and throat specialist Dennis Kraus of Lenox Hill Hospital in New York, who wasn’t involved in the paper.
Walsh, who practices at the University of Iowa Hospital, said the woman had gone for a nasal test ahead of an elective hernia surgery, and afterward noticed clear fluid coming out of one side of her nose.
She subsequently developed headache, vomiting, neck stiffness, and aversion to light, and was transferred to Walsh’s care.
“She had been swabbed previously for another procedure, same side, no problems at all. She feels like maybe the second swab was not using the best technique, and that the entry was a little bit high,” he said.
In fact, the woman had been treated years earlier for intracranial hypertension — meaning that the pressure from cerebrospinal fluid that protects and nourishes the brain was too high.
Doctors at the time used a shunt to drain some of the fluid and the condition resolved.
But it caused her to develop what’s called an encephalocele, or a defect at the base of the skull which made the brain’s lining protrude into the nose where it was susceptible to rupture.
Brain computed tomographic image from 2017 in the coronal and sagittal planes demonstrating encephalocele situated over the fovea ethmoidalis prior to nasopharyngeal testing for COVID-19. Sullivan, et al/JAMA Otolaryngology–Head & Neck Surgery
This went unnoticed until old scans were reviewed by her new doctors, who carried out surgery to repair the defect in July.
She has since fully recovered.
Walsh said he believes the symptoms she developed were a result of irritation to the lining of the brain.
If the problem hadn’t been treated, she could have developed a potentially life-threatening brain infection from bacteria that traveled up the nose.
Or, air could have entered the skull and placed excess pressure on the brain.
Most testing protocols call for clinicians to follow the path of the floor of the nose, which lies above the roof of the mouth, rather than pointing the swab up — or if they point it up, to do so with great care.
Walsh said that though this was likely a very rare occurrence, it was a reminder of the need for high-quality training, given that hundreds of millions more tests will be performed before the pandemic is over.
Let’s read this again:
But it caused her to develop what’s called an encephalocele, or a defect at the base of the skull which made the brain’s lining protrude into the nose where it was susceptible to rupture.
Jarrett Walsh, head and neck surgeon
update: Another report of a woman leaking spinal fluid after a covid test. Experts say it’s rare, but they aren’t surprised it happened.
From Fox29 TV, SAN ANTONIO (WOAI/KABB February 27th 2021)
A San Antonio woman is still in shock after she says a Covid nasal swab test went horribly wrong.
“It hurt, it was an immediate instant migraine,” says Chari Timm. “I’ve never had a migraine ever in my life.”Volume 90%Chari Timm says the swab was inserted in her nose and she instantly felt pain.
Chari was in need of a heart diagnostic test and protocol states she had to test negative for Covid before they could run any tests. She says the swab was inserted in her nose and she instantly felt pain.
“It started from the back of my head and just extend it to the front of my head and my entire brain was an extreme pain,” she says. “Instantly fluid just was leaking out of my nose.”
Chari was leaking spinal fluid.
A neurologist from Methodist and an ear, nose and throat doctor diagnosed her with pneumocephalus days later.
Pneumocephalus is when there has been a rupture in the dural membrane, or the lining that’s around the brain, which allows air to enter the space that’s normally occupied by the head.
Experts say it’s rare, but they aren’t surprised it happened.
“Patients are asked to tilt their head back and the trajectory is more parallel to the nostril, the bridge of the nose and that’s what can bring the that swab further up and put you in a range of potentially having that Covid swab then rupture the dural membranes,” says ENT specialist Spencer Payne.
Fortunately, there is a procedure to fix the hole, that would be a laparoscopy.
While it’s unlikely it’ll happen to you , if you feel uncomfortable when getting swabbed, speak up.
“It’s important that swab be directed as straight back as possible,” says Payne. “Patients should be empowered to understand that anatomy and direct their care if they think their swab is going in the wrong direction.”
If the brain can protrude into the nose, the swab certainly can breach the blood brain barrier, even if only indirectly.
Check the highlighted area in the figure above, the circled area is the access gate. That’s not soft tissue, but it’s far from a really resistent and insensitive one. You don’t need to go through it to cause harm to the brain, more or less directly.
“There are three layers of protection in the nose. There’s the mucosal lining which covers the inside of the nose. There’s the olfactory epithelium (involved in sense of smell). The inside, the dura mater, which means ‘tough mother,’ is a tough lining of skin around the brain. It’s hard to penetrate through (it) without something sharp,” said Dr. Shawn Nasseri, an ear, nose and throat surgeon in Los Angeles, in an interview with USA TODAY. (“Resurch” done on the toilet bowl).
Protrusion is one of their own typical straw-men, not the point they’re claiming to invalidate. It’s never been about protrusion. And “hard” doesn’t mean impossible. Same as in almost every fact-checker blog post (that’s all they are), they don’t even argue what they calim they do, but own fabrications.
“Increases in blood-brain barrier permeability occur and can be maintained with increasing inflammatory and oxidative and nitrosative stress being the initial drivers”, according to top Australian and Canadian researchers. All you need to do is to introduce the right agents in the right area,
Bottom line: the Covid-19 nasal test swabs, which are not used nasally at all, may not be able to easily protrude all the way to the brain blood barrier directly, but they certainly have the potential to get there or close enough, hurt and cause inflamations that can further leade to the “leaky brain” disease.
What Is the “Leaky Brain” and how it affects health
We took advice on this from Peter Smith, who specialises in treating and coaching people how to live well with mental health problems, digestive health problems/IBS, sleep problems and type II diabetes using natural therapies. He used these techniques to overcome and live well with his own bipolar disorder, IBS, he also briefly had and reversed type II diabetes. You can read about his mental health recovery story here.
The blood-brain barrier is a specialist membrane that surrounds the brain, it’s supposed to prevent toxins, bacteria and foreign proteins such as gluten from entering the brain. When the blood-brain barrier allows undesirable substances to enter the brain it can trigger inflammation that can damage key structures in the brain involved in depression, bipolar and other mental health problems; it can also cause a ‘foggy’ brain. In this section I’ll tell you how you can test the health of your blood-brain barrier and if it leaky how to fix it.
How to test the integrity of your blood-brain barrier
You can perform a basic test on your blood-brain barrier yourself at home, you can buy the neurotransmitter GABA as a supplement and take 1000 mg in the evening when you’re not going to go out or drive a car. When you take a GABA supplement and it is absorbed from the digestive system into the systemic blood it should not be able to get into across the blood-brain barrier and enter the brain; this is because the GABA molecule is very slightly too large to pass through a healthy blood-brain barrier.
When the blood-brain barrier (BBB) is excessively permeable or leaky however GABA from supplements can cross the BBB and will cause a rapid rise in GABA levels in the brain. Most people would experience this as a noticeable feeling of relaxation, sedation and a reduction in feelings of anxiety however paradoxically some people actually experience a temporary increase in anxiety or even a feeling of panic, this can be because their GABA synapses and pathways are already at the point of exhaustion and even a little bit of increased stimulation quickly leads to a temporary exhaustion and depletion. If you experience this paradoxical reaction because your GABA pathways are at the point of exhaustion you may initially respond badly to treatments aimed at increasing GABA activity in the brain, the solution is to aggressively reduce neuro-inflammation (inflammation in the brain) by treating any and every source of inflammation, see how to reduce neuro-information.
In terms of the GABA challenge test the important point is if feel any of the above effects it implies you have a leaky brain and you should fix it.
If you pass the test i.e. don’t feel anything on 1000 mg I would actually repeat the test the following night with 1500 mg just to be doubly sure. Do not engage in anything that you wouldn’t do if you were under the influence of alcohol or sleeping pills like drive a car during the test, ideally do the test in the evening just in case it produces a strong relaxation effect so that you have ample time to sleep it off overnight.
If you fail the GABA challenge test above you should not keep taking GABA because of the risk that repeatedly flooding the brain with GABA could desensitise your GABA synapses, the balanced way to increase GABA is to take substances like ashwagandha and theanine that readily pass the blood-brain barrier and stimulate the brain to make its own GABA and lithium orotate and passionflower that increase GABA sensitivity by increasing receptor sites within GABA synapses. See GABA Deficient Anxiety
A personal anecdote is I used to occasionally take GABA to sedate my brain counteract bipolar hypo-mania long before I knew that GABA should not be able to cross the BBB and that it could be used as a test the health of the blood-brain barrier. I found that GABA did work for me but was unpredictable, sometimes producing strong sedation and other times no noticeable effects at all. I now understand that this means the health of my blood-brain barrier was borderline and when the level of inflammation in my body was elevated my blood-brain barrier was leaky enough to allow GABA from supplements to enter my brain and other times my blood-brain barrier worked should; today GABA has no effect on me.
The importance of the blood-brain barrier in mental health
The blood-brain barrier is a protective membrane that separates the brain from the rest of the blood in the body, its job is to prevent unwanted substances from entering the brain. When healthy the blood-brain barrier blocks everything except nano-sized particles and a few desirable larger molecules are specifically allowed to pass through, even antibodies made by our own immune system are too big to pass through the blood-brain barrier, so the brain has its own separate immune system; furthermore the blood-brain barrier can make it difficult to administer medicines both pharmaceutical and natural to the brain, in my line of work I always have to ask the question does this medicinal substance cross the blood-brain barrier.
By and large the blood-brain barrier prevents viruses and bacteria from entering the brain, this is why infections in the brain are actually quite rare; some notable exceptions to this are the bacteria that cause meningitis, syphilis and Borrelia that causes Lyme disease, these smart pathogens release inflammatory chemicals called cytokines that cause inflammation and increased permeability in the blood-brain barrier to gain access to the brain.
The blood-brain barrier also prevents many toxins and pollutants from entering the brain it does not however do a good job of preventing toxic metals such as mercury[i], lead or cadmium from entering the brain.
Mercury is a highly penetrating substance, a dentist that specialises in safe amalgam filling removal once told me that the mercury vapours released when you drill an amalgam filling can penetrate a man-made rubber dam during the drilling process, inhaled and absorbed, which led to the development of new safer extraction techniques.
Besides obvious things such as bacteria and viruses the blood-brain barrier should keep toxins, pollutants and large half-digested food molecules such as gluten from wheat out of the brain. Our digestive system attempts to break down large protein molecules into individual amino acids (the building blocks of proteins), we then absorb the amino acids and build up into human shaped proteins but the process of breaking down foreign proteins into amino acids is never hundred percent complete or successful resulting in half-digestive protein molecules and strings of amino acids. Ideally the walls of our digestive tract should not allow these half digestive protein molecules to enter the bloodstream but when the walls of the digestive tract are excessively permeable then half-digested proteins pass through into the blood, this is sometimes called leaky gut syndrome. If the blood-brain barrier is also leaky then the half-digested proteins can make it all the way from digestive system into the brain and trigger the brains immune system and inflammatory response. Generally treating a leaky blood-brain barrier should go hand-in-hand with treating a leaky gut.
The role of hidden neuro-inflammation in mental health
The people mcking your “Google Univeristy diploma”. I’ve seen vlogs by 17y olds that look and sound better than Factcheck.org
There’s a growing understanding that mental health problems including depression, bipolar syndrome, OCD and anxiety are caused by diminished function in specific parts of the brain that control mood and mental health. In the affected areas there is literally a loss of synaptic connections and inflammation is thought to be the primary factor that causes this; a loss of serotonin carrying synapses in the limbic system that controls our mood for example result in depression. This is the new BDNF hypothesis of what causes mental health problems.
It can be very upsetting to hear that you may have a loss of synapses in your brain, so let me immediately reassure you that the brain is constantly remodelling itself losing and growing new connections this is called neuroplasticity and it can be stimulated and increased so you can regrow and repair the function in the affected parts of your brain. To learn how to do that see: How to regenerate your broken brain One of the key goals to achieve to increase neuroplasticity and overcome a mental health problem is to eliminate neuro-inflammation.
A leaky blood-brain barrier is not the only thing that can cause neuro-inflammation, other things that can independently cause neuro- inflammation include a pro-inflammatory diet, elevated cortisol production from overactive stress responses (a common finding in people with mental health problems), elevated blood sugar/insulin levels, drug and alcohol use although the latter also weakens the blood-brain barrier causing it to become leaky. Furthermore when a leaky blood-brain barrier is combined with leaky gut syndrome and an unhealthy bowel flora it increases the ability of the latter to cause neuro-inflammation.
In my practice a big part of my treatments is to eliminate neuro-inflammation by working on everything just mentioned.
Understanding inflammation
It’s common to think of inflammation is a bad thing but a short appropriate burst of inflammation is part of a healthy immune response, inflammation helps the affected body part to fight infection, clear toxins and repair itself.
Inflammation can exist in an extreme form with tell-tale signs including swelling, fever, pain and clinical markers such as elevated CRP in the blood; in the brain extreme inflammation is extremely dangerous and should be treated immediately with aggressive anti-inflammatory drug therapy such as steroids.
Alternatively inflammation can exist in a low-level in the background without producing any obvious signs this can be referred to as hidden inflammation; one of the big problems with low-level background inflammation is that it hidden and so may persist unnoticed for years chipping away at the health of your brain. When hidden inflammation persists over a long period of time it can damage key parts of the brain that control mood and cause at least contributes to mental health problems. Hidden inflammation can also be a central component of degenerative diseases including dementia and Alzheimer’s disease. For more information inflammation see: How to Reduce Neuro Inflammation to Treat Depression and Mental Health Problems
The brain has a separate hyper-sensitive immune system
Two important things to note about the brains immune/inflammatory response are firstly because the brain is so important it’s defensive immune/inflammatory responses are very easily provoked and secondly once provoked they remain active for a very long time. The combination of features is why a leaky blood-brain barrier can be so detrimental, for example just a small seemingly benign provocation from the entry of gluten into the brain can provoke neuro-inflammation that could last for days; gluten is notorious for being able to provoke a particularly aggressive immune/inflammatory response. I recently treated a patient who identified wheat is a clear trigger for her bipolar mania.
When we have a leaky blood-brain barrier and leaky gut syndrome the immune/inflammatory response may switched on literally every time we eat from half-digested foreign proteins entering the brain; the result would be continuous persistent neuro-inflammation wreaking havoc on delicate brain structures.
There’s also growing evidence that the toxins produced by an unhealthy bacterial colony in our intestines can be a significant contribution to neuro-inflammation if they are allowed to enter the brain, there are often so many supplements to take when you’re using natural therapies to improve a mental health condition that is easy to overlook the health of the bowel flora but it can have a significant effect and it’s worth taking probiotic supplements.
A personal anecdote is that for many years I used to eat wheat once a week, if I ate it twice a week I would get a pressure headache at the back of my head feel very slightly depressed and very grumpy; at that time I didn’t understand the significance of this and for over a decade enjoyed my one sandwich a week. I now understand that that one serving of wheat provoked inflammation in my brain that lasted several days and if I had a second serving of wheat before the inflammation from the previous serving had completely subsided the inflammatory effects were combined and compounded on top of each other to produced sufficient neuro-inflammation to give me a headache and psychological symptoms. Looking back I regret provoking low-grade hidden inflammation in my brain for several days each week. Today I avoid wheat and use rye/spelt bread made with sourdough rather than modern yeast which as far as I can tell does not produce any neuro-inflammation, I follow an anti-inflammatory diet and I have improved the health of both my digestive tract and blood-brain barrier.
What makes the blood-brain barrier become leaky?
The main thing that makes the blood-brain barrier become too permeable or leaky is inflammation in the blood-brain barrier itself. Just to be clear inflammation in the blood-brain barrier causes the blood-brain barrier to become too permeable or leaky which then allows undesirable substances to enter the brain which then triggers the brains defensive immune/inflammatory response and this results in increased neuro-inflammation.
The blood-brain barrier is just another part of the body and when there is widespread systemic-inflammation in the body in general it can inflame the blood-brain barrier and therefore from a practical treatment point of view to heal a leaky blood-brain barrier we have to eliminate systemic-inflammation throughout our whole system. Systemic-inflammation can be caused by a poor pro-inflammatory diet, over-active stress responses, pollution, toxins from and friendly bacteria in the intestines, leaky gut syndrome, allergies, autoimmunity, et cetera.
Alcohol and yeast overgrowth (Candida)
Excessive consumption of alcohol specifically weakens the blood-brain barrier because one of the breakdown products of alcohol is acetaldehyde and this specifically damages the blood-brain barrier. Acetaldehyde is also produced from yeast (Candida) overgrowth, the worst thing in the diet to promote the overgrowth of yeast is sugar. I have a question if anyone can answer this for me: does yeast overgrowth produce acetaldehyde by fermenting sugar in the blood into alcohol and then the alcohol breaks down into acetaldehyde or is the acetaldehyde produced independently of alcohol production and breakdown?
The clinical significance here is that if you have abused alcohol and or you have a yeast/candida overgrowth you should suspect you have a leaky blood-brain barrier and treated just in case.
How to heal a leaky blood-brain barrier
As just mentioned above systemic-inflammation in the body is a primary cause of a leaky blood-brain barrier, the practical implication of this is that the key thing to do to heal a leaky blood-brain barrier is reduce systemic-inflammation.
Two really big things to do to reduce systemic-inflammation are:-
Follow the anti-inflammatory diet and
Dampen down overactivity in the HPA axis.
Additional measures to reduce systemic-inflammation and heal the BBB include:-
Drink no alcohol for the duration treatment.
Eliminate leaky gut syndrome by following the anti-inflammatory diet and if necessary treating and eliminate SIBO (small intestine bacterial overgrowth) and intestinal yeast (Candida) overgrowth
Improve the condition of your intestinal microbiota (the bacteria) primarily with a diet containing a large amount of diverse polyphenols and fibre, if necessary thoroughly cleanse the bowels first then repopulate with friendly bacteria.
Consume copious amounts of chicken stock, this promote regeneration of both the blood-brain barrier and the intestinal wall. See How to Make a Healing Chicken Stock
Remove amalgam fillings from your teeth and detoxify heavy metals
Eat organic foods because they contain less pesticide residues.
Improve the quality of your sleep, because sleep deprivation particularly inadequate the rapid eye movement sleep that occurs in the second half of the night when we dream and learn new memories has been shown to degrade the integrity of the BBB[ii][iii]. For techniques on how to improve your sleep see my book: Sleep Better with Natural Therapies by Peter Smith available from Amazon.
Improve your oral hygiene, particularly your gum health with regular flossing and if necessary the use of the new oral pro/friendly bacteria lozenges. Believe it or not oral bacteria can be a significant source of inflammation in the body, if you have poor gum health consult with an oral hygienist before embarking upon the use of dental floss to avoid initially releasing dangerous bacteria into your bloodstream.
Supplements to heal a leaky blood-brain barrier
Only a few supplements are known to specifically improve the health of the BBB they include acetyl-L-carnitine, a specific form of B5 called pantethine and melatonin.
Acetyl-L-carnitine boosts the production of antioxidant enzymes that protect and heal the BBB[iv]. Unfortunately there some studies have suggested that if carnitine is regularly consumed it feeds and builds up a particular bacteria in the intestines and these bacteria produce a chemical from the carnitine that damages our arteries; the suggestion is that the inherently high level of carnitine found in meat may actually be the mechanism whereby meat consumption increases the risk of heart disease. The evidence that this is the case still limited furthermore in the animal studies the form of carnitine look at was specifically L carnitine as opposed to acetyl-L-carnitine which can help heal the BBB, nevertheless I don’t recommend consuming something that could cause arterial damage and contribute to heart disease which is the leading cause of death in developed countries especially at high doses. I hope that further studies will show that acetyl-L-carnitine is not harmful to arterial health because carnitine is useful for depression, cellular energy, weight loss and healing the BBB.
Pantethine boosts the production of the key enzyme that clears acetaldehyde from the brain and therapeutic use of pantethine has been shown to strengthen the BBB so significantly it was able to prevent malaria from entering the brain (you can easily find references to this online).
Therapeutic doses start at 1000 mg twice a day with meals.
Melatonin besides being a potent free radical scavenger and inherently anti-inflammatory, melatonin has been shown to protect the integrity of the BBB, however the dosage used in the animal studies was enormous way beyond any human would supplement [v]. I’ve accumulated quite a lot of both personal and professional experience with the use of melatonin supplements, I have observed that at high doses above 2-3 mg many people experience a significant increase in the intensity their dreams even to disturbing levels and by personal experimentation one can work out a dosage that enhances and prolongs the rapid eye movement dreaming sleep phase.
Resveratrol is an antioxidant/polyphenols naturally occurring in foods such as red grapes, red wine and raspberries that has numerous health benefits especially the health of the brain, it has also appears to restore the integrity of the BBB and reduce neuro inflammation[vi].
High strength resveratrol is expensive, a good value for money resveratrol containing product I take myself and regularly prescribed Doctor’s Best French Red Wine Grape Extract 2 to 4 capsules a day, the same company also make quite good value resveratrol, if you are not limited by the expense Life Extension make very high quality resveratrol supplements; you can find all these products on iherb.com
Remember alcohol specifically weakens the blood-brain barrier so abstain from alcohol while you are treating a leaky BBB.
In addition to the above remedies I would recommend simultaneously taking high doses of antioxidants supplements that reduce systemic-inflammation to help create the conditions in the body conducive to repairing the blood-brain barrier.
My recommended combination:- Rutin Now Foods one capsule twice a day Ascorbyl palmitate 1000 mg twice a day Curcumin plus piperine (there are lots of curcumin products available but only very few deliver significant levels of curcumin to the brain) I recommend Super Bio Curcumin from Life Extension with a separate piperine. Vitamin E (gamma E) 400 IUs twice a day Alpha lipoic acid 150 to 600 mg twice a day NAC cysteine 1200 mg once or twice a day.
REFERENCES:
[i]American Chemical Society. “Mercury Can Jump Barrier That Keeps Toxins Out Of Brain.” ScienceDaily. ScienceDaily, 9 September 1999. <www.sciencedaily.com/releases/1999/09/990909080318.htm>.[ii] J Immunol Res. 2016;2016:4576012. Epub 2016 Sep 21. Blood-Brain Barrier Disruption Induced by Chronic Sleep Loss: Low-Grade Inflammation May Be the Link. Hurtado-Alvarado G1, et.al. PMID: 27738642 PMCID: PMC5050358 DOI:10.1155/2016/4576012[iii] Sleep Restriction in Pairs Blood-Brain Barrier Function PMID: 25355222 PMCID: PMC4212067 DOI: 10.1523/JNEUROSCI.2111-14.2014[iv] Haorah J, Knipe B, Persidsky Y. Stabilization of superoxide dismutase by acetyl-l-carnitine in human brain endothelium during alcohol exposure: Novel protective approach. Free Radic Biol Med. 2011 June Department of Pharmacology and Experimental Neuroscience, University of Nebraska Medical Center, Omaha, NE 68198-5215, USA.[v] PLoS One. 2016; 11(5): e0154427. Published online 2016 May 6. doi: 10.1371/journal.pone.0154427 PMCID: PMC4859489 Melatonin Preserves Blood-Brain Barrier Integrity and Permeability via Matrix Metalloproteinase-9 Inhibition Himakarnika Alluri, Rickesha L. Wilson, et al[vi] Georgetown University Medical Center. “Resveratrol appears to restore blood-brain barrier integrity in Alzheimer’s disease ScienceDaily 27 July 2016.
Leaks in Brain May Contribute to Dementia
Study finds blood vessels in older adults break down, age-related blood vessel leaks in the brain may contribute to the development of Alzheimer’s disease and other types of dementia, according to a 2015 study.
The findings suggest it may be possible to use brain scans to detect such leaks and repair them in order to prevent damage that can lead to dementia, the University of Southern California researchers said.
The investigators analyzed contrast-enhanced brain images from 64 people of various ages and found that the brain‘s protective blood barrier becomes leaky with age. This leakage begins in the hippocampus, an important learning and memory center damaged by Alzheimer’s disease.
“This is a significant step in understanding how the vascular system affects the health of our brains,” said lead investigator Dr. Berislav Zlokovic, director of the Zilkha Neurogenetic Institute at the university’s Keck School of Medicine.
“To prevent dementias including Alzheimer’s, we may need to come up with ways to reseal the blood-brain barrier and prevent the brain from being flooded with toxic chemicals in the blood,” Zlokovic added in a university news release.
The study was published Jan. 21 in the journal Neuron.
Post-death examinations of Alzheimer’s patients’ brains reveal damage to the blood-brain barrier. However, why and when this damage occurs is unclear, the researchers noted.
About 5.2 million Americans have Alzheimer’s disease, the most common type of dementia. By 2050, about 16 million Americans over age 65 will have dementia, according to the Alzheimer’s Association.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
It’s all in the meme that stands as cover for this post. We published it on some socials a bit over 24h before Trump’s latest endorsement of Covidiocracy aka The Big Reset. No, this is not gonna be one of those long intricate investigations, that’s all there is to it. I could develop a bit, but honestly, if you don’t pick it up from the meme, you won’t pick it up from the meme explanations. I’m going to leave a few more hints below, though.
When we felt most badass, someone pulled our sleeve: there’s a demi-god on the webs! We know nothing more as of now, except that he’s a very militant Trump-hater. The only question: prediction or pre-science? Either way, as spectacular as logical, it’s the details that are very striking. Ours was an anticipation based on following trends and joining dots:
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
People started to think the meme it’s just that, as no one seemed to get a hold of the paper in either physical or digital form. We have found the whole publication on archive.org, in PDF, Download right here ! Regardless of our opinions on the content, this is part of the popular culture .
Depopulation Through Forced Vaccination:
The Zero Carbon Solution
By Rachel Windeer. (First published June 2011 in Issue 4 of The Sovereign independent)
On April 26th, 2009 the Irish Independent published an article titled ‘Concern for Children’s Health as Parents ignoring vaccines’. Edel Kennedy, you should be ashamed of yourself! This is nothing less than an attempt by government, through their puppets in the media, to remove the rights of parents to determine the life choices of their offspring and removes any doubt that we now live in a dictatorship.
This is an OUTRAGEOUS insult to every parent in the country who has the common sense to research the efficacy of vaccines themselves by simply looking at the historical record rather than trust politicians whose lies in the media, including those perpetrated by the Dept. of Health under Mary Harney regarding the farce of ‘ swine flu’ and the dangerous myth of HPV vaccination, have led the country into the abyss of utter poverty and sold the country into the communist grasp of European bureaucrats whose sole aim is the destruction of every member nation’s sovereignty leaving them clutching at the bailout begging bowl of the IMF.
Vaccines are a fraud; pure and simple!
The historical record PROVES this for anyone with a little patience and the courage to investigate the FACTS for themselves, and it does take courage, especially for those in the medical profession whose careers will be at risk if they dare expose this danger to our children. It also shatters their illusions that they’re part of an organization which is far from beneficial to those they believe they’ re protecting from illness. However, their Hypocratic Oath should compel them to investigate such wild claims put out by pharmaceutical giants and their drug dealer sales representatives instead of taking the word of an industry well known as being utterly corrupt and ruthless in its business practices.
The Irish haemophiliac scandal, where patients were knowingly infected with HIV through contaminated blood products should be enough to convince anyone of Big Pharma’s murderous intent. This brings us to the real reasons for vaccinations. I’m not even going to prove to readers that they don’t work. I’ll simply urge you to look up the historical record. One simple example is the demise of measles.
The measles death rate had declined by 98% from 1915-1958 prior to any vaccination being introduced.
In 1988 and 1989, 69% and 89% for measles cases in American school-aged children had been vaccinated.
In 1995, 56% of ALL measles cases in America were vaccinated.
These figures come from medical journals. Those 3 simple examples PROVE that unvaccinated children are less likely to contract measles and that the vaccine was useless. Look that up for yourself. All other vaccine claims that they’ve cured or eliminated disease follow a similar pattern. Better hygiene, clean water and good healthy food was the cause of the decline and any doctor worth his smelling salts should know that. If they don’t then they are misinformed on a grand scale or they’re in complete denial. Therein lies the problem. Why have doctors been ‘indoctrinated’ to believe that vaccines are the sacred cow of medicine when the historical record clearly shows that they are virtually useless?
Hold onto your sanity because I have some bad news for you.
The real reason for vaccinations, apart from the massive profits to the manufacturers, is to ensure that you get sick throughout your life, again not only to enrich these same corporations that made you sick, but to ensure that many, if not all of you, die before you ever receive your pension and when you are no longer any of use to society. That’s why they want you retiring later in life and are forcing you through economic terrorism to work longer regardless of your age or health. They literally want to work you to death. If you don’t work you will be classed as a burden to society, a financial cost which society has to bear, and therefore you will be stigmatised as a ‘useless eater’; a consumer of resources needed for the rest of society. When Big Pharma can no longer profit from the illness they gave you, you will be left to die.
This is the depopulation agenda promoted under the United Nations Division of Population under the Department of Economic and Social Affairs. We only need look at Africa, the nation which the United Nations has said themselves, could feed the world. Why then are millions in Africa starving to death on that continent? It’s meant to be that way folks.
All of us at one time or another have been led to believe in the efficacy of vaccines. I was one of them and had my child vaccinated nearly 35 years ago. I wouldn’t even dream of it now. I think it’s safe to say that we’re all aware of the real pandemic, as opposed to the fake pandemics of the past. It’s called ‘CANCER’. Autism is also at crisis (pandemic) levels all across the world where mass vaccination programs exist.
Prior to mass vaccination, cancers were extremely rare, as in almost nonexistent. Today in the western, so called developed world, we face a crisis of cancer to the extent that between one in five to one in two will suffer, many dying, from one form of cancer or another. What’s happened to cause this pandemic?
We only have to look back at the Jonas Salk polio vaccine that went around the world in the full knowledge that it contained the SV40 virus which had no other purpose than causing cancer; yet it was pushed as a vaccine for polio when, as with measles, polio was well in decline prior to any vaccine due to the same factors.
Enter stage right at the TED 201 0 conference, Mr. Bill Gates, head of Microsoft, the biggest computer firm on the planet. What has Bill Gates to do with vaccines you’ re wondering?
See the quote in the image above. Those are his EXACT words. Are you beginning to get the picture?
The globalist elite care nothing for humanity; ordinary men, women and children must be eliminated in their delusional minds to ensure that their superior types go into the future with the best of breeding being the only criteria worthy of saving. You and I are no longer required and that is why we are seeing the loss of our economy, our wealth, our health, our happiness and ultimately, OUR LIVES
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
This article is as old as 2010, but no one has ever heard of any actual progress on these issues since, so it’s as good as fresh off the press. It originally appeared with a different title, as seen below. Christopher Lane, Ph.D., has won a Prescrire Prize for Medical Writing and teaches at Northwestern University. He is the author of Shyness: How Normal Behavior Became a Sickness. – S.m
Ghostwriting and Medical Fraud
Can any medical research studies be trusted?
Banner at the March for Science 2017, Washington, D.C. Photo: becker1999 @ Flickr
“Much of what medical researchers conclude in their studies is misleading, exaggerated, or flat-out wrong,” writes David H. Freedman in November’s Atlantic Monthly. “So why are doctors—to a striking extent—still drawing upon misinformation in their everyday practice?”
Freedman’s hard-hitting article, “Lies, Damned Lies, and Medical Science,” concentrates on the work and findings of Dr. John Ioannidis, a medical professor in Greece who has “spent his career challenging his peers by exposing their bad science.” Far from being dismissed as a maverick or crank, Dr. Ioannidis is highly sought after. “His work has been widely accepted by the medical community,” Freedman writes. “It has been published in the field’s top journals, where it is heavily cited; and he is a big draw at conferences.” One of his articles for PLoS Medicine, on bias in clinical trials, is the most downloaded in the journal’s history.
The real shock of Dr. Ioannidis’ work? He charges that “as much as 90 percent of the published medical information that doctors rely on is flawed.”
The Greek professor’s underlying goal, the Atlantic reports, is to shed an uncompromising spotlight on just how often—and how much—drug companies have been “manipulating published research to make their drugs look good.” This issue was, you may recall, the subject of my last post, following news that the Public Library of Science (PLoS) and New York Times had successfully lobbied for the release of 1,500 documents that the drug-maker Wyeth commissioned to boost its spotty product, Prempro. Prempro, a Hormone Replacement Therapy (HRT), has been shown to increase women’s risk of breast cancer, stroke, and dementia. Beyond that, the journal and newspaper discovered that Wyeth not only had fabricated evidence about its treatment, but also had paid a ghostwriting agency to create and plant vast amounts of that “evidence” on the drug-maker’s behalf. (The documents are freely available here.)
To the evidence uncovered by the Atlantic, Guardian, New York Times, and PLoS, we can also add GlaxoSmithKline’s highly incriminating document CASPPER, short for “Case Study Publications for Peer Review,” which the drug-maker seems to have chosen as the name of its shell company because it brought to mind the cartoon ghost Casper, as in “CASPPER, the friendly ghost-writing agency.”
A confidential brochure published by GSK’s Philadelphia office and circulated “for consultant use only,” CASPPER makes clear that the drug maker’s “PAXIL Product Management” team had “budgeted for 50 articles in 2000″ (p. 11). That was the year, incidentally, the corporation spent more than $92 million on an ad campaign to promote social anxiety disorder, following the medical truism that one must first sell the disease before pitching the product advertised as treating it. Among other things, the CASPPER brochure indicates a strong preoccupation with devising and planting favorable articles about Paxil, the first of the SSRI antidepressants to be given an FDA license for the treatment of social anxiety disorder (March 1999). Other confidential documents that colleagues have sent me indicate that GSK internally was concerned about 1-in-5 patients reporting significant side effects from Paxil within weeks of starting treatment on it in their clinical trials.
According to the Associated Press, which covered this scandal when it broke last year, GlaxoSmithKline “used [the] sophisticated ghostwriting program to promote its antidepressant Paxil, allowing doctors to take credit for medical journal articles mainly written by company consultants.” “Manuscript preparation can be a time-consuming task,” the company recognizes in its brochure, while “CASPPER coordinates these responsibilities for contributing physicians” (p. 8).
Working with professors and researchers with names in the field, even to the point of mimicking their personal styles, CASPPER committed to crafting positive-sounding data in such a way that the professor would be willing to add his or her name to the fabricated article. After dogged effort targeting and revising for journals, the shell company would then be responsible for placing said article in prominent publications.
According to Policy and Medicine, “Articles from the company’s [ghostwriting] program [did indeed] appear in five journals between 2000 and 2002, including the American Journal of Psychiatryand the Journal of the American Academy of Child and Adolescent Psychiatry.”
In the case of Wyeth and GlaxoSmithKline, who’ve been caught red-handed with their ghostwriting agencies, the fabrication of medical evidence amounts to widespread, certifiable fraud. A spokeswoman for Glaxo’s London office even is on record as saying, “The published articles noted any assistance to the main authors,” which is supposed to sound reassuring, I guess, though readers of the American Journal of Psychiatry expecting good data clearly wouldn’t have known the extent of the drug company’s involvement in crafting more or less the entire article. The same spokeswoman is quoted as adding that the ghostwriting program “was not heavily used and was discontinued a number of years ago.”
So we can all breathe a sigh of relief that medical fraud is over, right? Wrong. For starters, there’s Wyeth’s 1,500-document ghostwritten archive, which the drug company has been required to make available to the public. The Wyeth Ghostwriting Archive constitutes an example of medical fraud on a massive scale.
According to the Guardian, moreover, DesignWrite, the medical communications company that Wyeth hired, “boasts that over 12 years they have planned, created, and/or managed hundreds of advisory boards, a thousand abstracts and posters, 500 clinical papers, over 10,000 speakers’ bureau programmes, over 200 satellite symposia, 60 international programmes, dozens of websites, and a broad array of ancillary printed and electronic materials.”
And what about seemingly milder infractions and distortions of evidence?
“Wasn’t it possible,” Dr. Ioannidis is reported as asking his colleagues in the Atlantic article, “that drug companies were carefully selecting the topics of their studies—for example, comparing their new drugs against those already known to be inferior to others on the market—so that they were ahead of the game even before the data juggling began? Maybe sometimes it’s the questions that are biased, not the answers.”
“Though the results of drug studies often make newspaper headlines,” concludes Freedman at the Atlantic, “you have to wonder whether they prove anything at all. Indeed, given the breadth of the potential problems raised at the meeting, can any medical-research studies be trusted?”
It’s a bleak and troubling question, and in his last post for “Mad in America,” his excellent PT blog, Robert Whitaker came last week to the same conclusion:
“Research in this country is financed by pharmaceutical firms that can’t be trusted to conduct honest science.”
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
“Bill Gates and Congressman Bobby L. Rush are not involved in acts of corruption regarding the Trace Act because they say so”. This is USA Today’s lame attempt to wash and suppress the latest Bill Gates – Rockefeller – Covid-19 scandal. They are Facebook’s prime fact-checkers. They decide what pages and links get shadow-banned or deleted. And a trove of publicly available documents prove they lie through their teeth (again).
In Covidiocracy, fact-checking is as easy as “Our people are innocent because they so, if you argue we shut you down”. It totally doesn’t sound like the communist narrative-enforcement I’ve witnessed in communist Romania 30 years ago, sure…
Facts need to be checked from three independent sources before publishing.
Rule #0 in true Old Normal journalism
Here are more than four sources:
US House of Representatives attest that Democrat Congressman Bobby L. Rush and his spouse visited Rwanda in 2019 with funding from Bill Gates and the Rockefellers, among others. (Download PDF)
Rush was a participant in the Aspen Institute Congressional Program for Africa’s Economic, Security, and Development Challenges and the U.S. Role, which took place August 12-19, 2019 in Kigali, Musanze, and Muhanga, Rwanda. There were seven other participants from the U.S. Congress, all of whom were Democrats from CA, IL, NY, and MO, except for Republican Fred Upton from Michigan, who was the former chairman of the committee on energy and commerce.
2. Aspen Institute‘s own event presentation (Download PDF) attest that there were a handful of speakers in attendance, including Madeleine Albright who served under President Bill Clinton and received a Presidential Medal of Freedom from President Barack Obama, Peggy Clark who received a presidential award for excellence in microenterprise from Bill Clinton, and Mary Robinson the former President of Ireland from 1990-1997 who also received a Presidential Medal of Freedom from President Barack Obama.
Who else was in attendance? Dr. Paul Farmer from Partners in Health who is running a massive scale contact tracing program in multiple states, two representatives from the Bill & Melinda Gates Foundation, and a dozen other scholars.
Another scholar at this event Bobby Rush attended, that was funded by Bill Gates and friends, was Dr. Jonathan Epstein who is the Vice President for Science and Outreach of EcoHealth Alliance, founded in 1971. He is a veterinarian and disease ecologist who studies emerging zoonotic viruses such as Nipah and Ebola, along with SARS, MERS, and coronavirus. His specialty is bats. “In 2004, Dr. Epstein was part of a team of Chinese, Australian, and American scientists that identified horseshoe bats as the natural wildlife reservoir for SARS coronavirus in China. He also worked on the first team to investigate animal reservoirs of MERS coronavirus in Saudi Arabia, following its discovery in 2012.”
The best independent media report I’ve found on this, by Corey Lynn, points out that EcoHealth Alliance is the non-profit that received the $3.7 million NIH grant back in 2014 to study the coronavirus and had been working with the Wuhan Institute of Virology. EcoHealth Alliance’s President Dr. Peter Daszak said that none of the funds were given to the Wuhan Institute, but after Trump raised concerns, NIH contacted EcoHealth and instructed them to halt spending the remaining grant and that they were pulling their five-year grant that was just reauthorized in 2019. Daszak also stated that EcoHealth was spending $100,000 a year to collaborate with the Wuhan Institute, which was always preapproved by NIH. They used a portion of the grant funds to run genetic sequences of two bat coronaviruses that they discovered, which have since been used as lab tools to test the antiviral drug Remdesivir.
EcoHealth works in nearly 30 countries studying emerging pandemic threats. They have over 20 science and policy advisors, including individuals from the National Institutes of Health, World Health Organization, CDC, and the Bill & Melinda Gates Foundation.
In addition to NIH funding, the EcoHealth Alliance has played a vital role in the ‘Emerging Pandemic Threats PREDICT-I’ and ‘PREDICT-II’ program with USAID, universities and other NGOs. This dates back to 2009. Between 2009-2018, $195 million has been disbursed and funds continue to be dispersed through 2020. In their Road to EPT-2 document, they state that EPT-1 was to support the World Health Organization, who is currently under investigation and the Trump administration has halted funding to them. They “targeted 25 laboratories in 20 EPT-2 focus countries for enhanced capacities in handling, diagnosing and characterization of known high consequence and novel viruses in wildlife (PREDICT and CDC).”
In 2018, while co-founder of Partners in Health Jim Yong Kim was the president of the World Bank, they released the ‘One Health Operational Framework for Strengthening Human, Animal, and Environmental Public Health Systems at Their Interface,’ with EcoHealth Alliance. This entire 152-page document is about ‘One Health,’ which originated out of a Wildlife Conservation Society conference at Rockefeller University in 2004, and its aim is to reduce risks of infectious diseases at the animal-human-ecosystems interface. It is a collaboration between the World Bank, WHO, UNICEF, CDC, FAO, OIE, other partners, NGOs.
Corey Lynn sums it up nicely for us, so far: “Bobby Rush has a long history of pay to play and disregarding paying taxes of any kind. Just last August, he traveled to Africa for an Aspen Institute congressional conference of approximately 45 individuals and spent time with Obama and Clinton award winners, Dr. Paul Farmer from Partners in Health who is currently running the contact tracing program in Massachusetts while his partner Jim Yong Kim is rounding up other states, Dr. Jonathan Epstein from EcoHealth Alliance who just had their NIH funding cut due to connections with the Wuhan Institute of Virology, and two representatives from the Gates Foundation, while the Gates, Rockefellers, Democracy Fund, and others paid toward the $19,000 dollar expense Rush incurred for this sponsored event. Nine months later, he introduced a bill to dispense $100 billion dollars to NGOs and other organizations to carry out home-to-home contact tracing throughout the country.”
3. Partners in Health put out a press releaseannouncing their new ‘contact tracing accompaniment unit’ which would “coordinate and harmonize” approaches across the country by PIH providing small teams of experts, advisers, collaboration, and online toolkits and materials for free. This occurred less than two weeks after Congressman Bobby Rush introduced H.R.6666 for $100 billion to NGOs for contact tracing,
They will be seeking grants, or shall we say taxpayer dollars, while their initial funding came from The Audacious Project, which is a collaborative funding initiative housed at TED that launched in 2018. Their partners include the Gates Foundation, Virgin Unite, Children’s Investment Fund Foundation, and about 20 others.
PIH is already supporting programs in Massachusetts, New Jersey, Ohio, North Carolina, as well as advising in California, Minnesota, and Maryland.
4. According to their own website, CDC Foundation partly funds CDC, the Trace Act coordinator, and is funded by Bill Gates and the Rockefellers, among many other corporate and private interests.
The CDC Foundation is the sole entity created by Congress to mobilize philanthropic resources to support CDC’s critical health protection mission.
Facts ruling: Public documents provided by US Congress, Aspen Institute and CDC prove that Bill Gates, among others, invested money in Bobby L. Rush in 2019, had contacts with him, and obtained benefits from Rush’s infamous HR. 6666 aka the Trace Act. Thus the tracing operation funded by the US taxpayers has never left Gates’ sphere of influence or his agenda. This is the definition for “corruption”. All of the above also prove that Facebook’s fact-checkers are a laughable bunch of braindead unprofessional clowns, manipulators-wanna-be, with no other qualities than the money, technology and monopolies propping them up. And these clowns decide which media gets shadow-banned or pushed upfront on world’s biggest Internet social anti-network. They can’t even make up a decent lie to wash Gates’ dirty undies, but they have the power to repeatedly turn off the lights on us. Unless you help us take that power from them by spreading the actual facts, and by confronting them everywhere you encounter them. Third, and most important conclusion is, on our scale, the strong indication of pre-science regarding the 2020 pandemic and the course of action that will be taken by US authorities one year later.
And this is how you fact-check, Facebook bozos! Ah, one more thing: “our research does not support this claim” does not equate “this claim is false”, dickheads. It only confesses your limits. You were supposed to prove it false, you just haven’t proved it true, because you’re not paid to by your sponsor, which happens to openly be Bill Gates’ long time supporter and collaborator. So you’re taking money for Gates’ proxies to smear Gates’ enemies, you filthy presstitutes!
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
According to the reputed truth-gods of Fb, Gates and WHO and the other Event 201 attendees spewed Rona conspiracies in a video they made in October last year, which implies pre-science and vindicates the people calling covid a “plandem1c”
Many revere and admire the elites for their grandiose plan to enslave the whole humanity, but in fact all their plan is dumb AF from its fundamentals down to its executives, and this is just one of the many evidences. I mean you want to control the world but you can’t even automate censorship on Internet and you end up shooting yourself in the both knees relentlessly? Imagine a fanfare of clowns with megalomaniac delusions, applauded by a congregation of geese. Covidiocracy is destined to cannibalise itself, starting with its propaganda machine, see the SJW/cancel culture.
I made this post very visual and simple so fact-checkers can understand it: They targeted us but it’s their people’s video and it’s made last year. We work mainly with their sources precisely because they’re dumb and predictable and we knew we’ll have to deflect back these BS attacks when they occur. And they fell right into it as soon as they could. They’re a buncha morons with too much money and too many toys.
Basically, Facebook and a host of its “fact-checkers” such as USA Today, Factcheck.org and more, have claimed that one of our latest video uploads “repeats information identified by independent fact-checkers [themselves] as false”.
Thing is we’re not the authors of the content, we just mirrored (reuploaded) a video from Johns Hopkins, untouched, we’re just platforming these people, Facebook told us they’re good credible people :D.
Original source, pls watch all their videos, preferably the mirrors on our channel so we can benefit, not these conspiracy theorists! 😉
So the authors of the missinformation in the video are, among others: WHO Bill & Melinda Gates Foundation World Bank World Economic Forum Johns Hopkins Lufthansa and many more
Bonus: the video has actually NOTHING, ZERO, 0 to do with the BS fact-checkers are munching there, it’s not about the man-made origins of the virus or anything like that. Remember:
It doesn’t matter what Facebook says
Silviu “Silview” Costinescu
I think Facebook’s combat style is called Fact-Fu
I don’t know it but I bet factcheck.org took money from Gates to label him as a conspiracy head.
Please watch and share our Facebook upload, if not to raise awareness, at least just to piss off these douchebags!
First hour of the simulation is already on our Bitchute, Youtube, we have a BrandNewTube channel too now. All full of “conspiracies”.
At least good thing Facebook and its “independent fact-checkers” are not mere narrative-enforcers and smear-machines 😀
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
It all comes round now… World leaders dealt above our heads, played their games and kept the plebs in the dark using smoke-screens of technocratic lingo. The elites are resetting our lives. All about The Great Reset.
We got encores from Henry Makow for this one, which is cool, because he is one of the early truthers who helped me when information was scarce and I was hungry.
TIMELINE
If you want to do a really good learning job, you start where it all started, about 150 years ago. Hosts are vetted historians and independent investigators:
2001 – The Dark Winter drills and the Anthrax attacks.
2005 WHO member countries sign the new International Health Regulations (IHR) which is basically the implementation of the Health Management chapter in The Great Reset, the tactical manual for the New World Order aka New Normal. The document envisions using drills to perfect the new system. Download IHR in PDF
Above: “Tom Inglesby, CEO and Director of the Center for Biosecurity of UPMC gives welcome and opening remarks for a one day conference, Improving Epidemic Response: Building Bridges Between the U.S. and China, held May 15, 2012, in Washington, DC. The conference focused on strengthening collaborative approaches between the U.S. and China to prepare for and respond to disease outbreaks”. – Center for Biosecurity of UPMC More info here
2014 – The creation of The Global Health Security Agenda (GHSA), “a group of 69 countries, international organizations and non-government organizations, and private sector companies that have come together to achieve the vision of a world safe and secure from global health threats posed by infectious diseases”. It was launched by a group of 44 countries and organizations including WHO, as a five-year multilateral effort with the purpose to accelerate the implementation of IHR, particularly in developing countries. In 2017, GHSA was expanded to include non-state actors. It was also extended through 2024 with the release of the Global Health Security Agenda (GHSA) 2024 Framework (called “GHSA 2024”). The latter has the purpose to reach a standardized level of capacity to combat infectious diseases. All financed through the World Bank, of course. Which is controlled by the Rothschild cartel.
Rothschilds patent the first Covid-19 test kit in the Netherlands. According to Dutch Government’s website for patent registrations: “A method is provided for acquiring and transmitting biometric data (e.g., vital signs) of a user, where the data is analyzed to determine whether the user is suffering from a viral infection, such as COVID-19. The method includes using a pulse oximeter to acquire at least pulse and blood oxygen saturation percentage, which is transmitted wirelessly to a smartphone. To ensure that the data is accurate, an accelerometer within the smartphone is used to measure movement of the smartphone and/or the user. Once accurate data is acquired, it is uploaded to the cloud (or host), where the data is used (alone or together with other vital signs) to determine whether the user is suffering from (or likely to suffer from) a viral infection, such as COVID-19. Depending on the specific requirements, the data, changes thereto, and/or the determination can be used to alert medical staff and take corresponding actions.”
Pirbright Institute patents an avian coronavirus vaccine for a SARS-COV-2 relative. Just for veterinary use, they say, because this is an animal virus. But so was SARS-COV-2 initially, wasn’t it? The Institute is named after a British baron from the Pirbright family who’s a direct descendant of Mayer Rothschild, it’s funded by the Wellcome Trust and Bill Gates, among others.
The Institute holds Patent no. 10130701 which covers the development of an attenuated (weakened) form of the coronavirus that could potentially be used as a vaccine to prevent respiratory diseases in birds and other animals. Many vaccines are made in this way, from flu to polio. We have not yet developed an IBV vaccine, but research is ongoing. The Institute is strategically funded by the Biotechnology and Biological Sciences Research Council, part of UK Research and Innovation (BBSRC UKRI) and also receives funding from many other organisations including the Bill & Melinda Gates Foundation. The patented work was not funded by the Bill & Melinda Gates Foundation. More information on The Livestock Antibody Hub which is funded by the Bill & Melinda Gates Foundation is available on our website.
Baron Solomon Benedict de Worms (1801–1882) was an Austrian aristocrat, plantation owner in Ceylon, and stockbroker in London.
Contents [show] Biography[edit] Early life[edit] Solomon Benedict de Worms was born on 5 February 1801 in Frankfurt.[1][2] His father was Benedikt Moses Worms (1769–1824) and his mother, Schönche Jeannette Rothschild (1771–1859).[1][3] He had two brothers, Maurice Benedict de Worms (1805–1867) and Gabriel Benedict de Worms (1802–1881), and one sister, Henriette Worms (1803–1879).[2][3]
His maternal grandfather was Mayer Amschel Rothschild (1744–1812), the founder of the Rothschild banking dynasty.[1] As a result, his maternal uncles were Amschel Mayer Rothschild (1773–1855), Salomon Mayer von Rothschild (1774–1855), Nathan Mayer Rothschild (1777–1836), Carl Mayer von Rothschild (1788–1855), James Mayer de Rothschild (1792–1868), and his maternal aunts, Isabella Rothschild (1781–1861), Babette Rothschild (1784–1869), Julie Rothschild (1790–1815) and Henriette Rothschild (1791–1866).[1]
Career[edit] After spending some time in London, he went to Ceylon to build one of the largest plantations there with his brothers Maurice and Gabriel.[2] In 1865, he returned to London and worked as a stockbroker.[2]
On 23 April 1871, Franz Joseph I of Austria (1830–1916) made him 1st Baron de Worms [Austria].[1][2] Three years later, on 10 August 1874, Queen Victoria (1819–1901) allowed him to use his Austrian title in Great Britain.[1][2]
He was a life member of the Council of the United Synagogue and a warden of the Great Synagogue of London.[2]
Personal life[edit] He married Henrietta Samuel, daughter of Samuel Moses Samuel, on 11 July 1827.[1] They had four children:
George de Worms, 2nd Baron de Worms (1829–1902).[1][2] Anthony Mayer de Worms (1830–1864).[1] Ellen Henrietta de Worms (1836-unknown).[1] Henry de Worms, 1st Baron Pirbright (1840–1903). –
And the youngest of his sons will give his name to the Pirbright Institute
2017-2018 – World Bank’s website reports massive shipments of COVID-19 medical devices (tests, mainly). See our previous reports.
2019 In its first annual report, WHO and WB’s Global Preparedness Monitoring Board identifies the most urgent actions required to accelerate preparedness for health emergencies. This first report focuses on epidemics and pandemics. The document is “co-convened by the World Health Organization and the World Bank Group”. Under “Progress indicator(s) by September 2020“, the report states:
The United Nations (including WHO) conducts at least two system-wide training and simulation exercises, including one for covering the deliberate release of a lethal respiratory pathogen. WHO develops intermediate triggers to mobilize national, international and multilateral action early in outbreaks, to complement existing mechanisms for later and more advanced stages of an outbreak under the IHR (2005).
Countries, donors and multilateral institutions must be prepared for the worst.
A rapidly spreading pandemic due to a lethal respiratory pathogen (whether naturally emergent or accidentally or deliberately released) poses additional preparedness requirements. Donors and multilateral institutions must ensure adequate investment in developing innovative vaccines and therapeutics, surge manufacturing capacity, broad-spectrum antivirals and appropriate non-pharmaceutical interventions. All countries must develop a system for immediately sharing genome sequences of any new pathogen for public health purposes along with the means to share limited medical countermeasures across countries.
The United Nations must strengthen coordination mechanisms.
The Secretary General of the United Nations, with WHO and United Nations Office for the Coordination of Humanitarian Affairs (OCHA), must strengthen coordination in different country, health and humanitarian emergency contexts, by ensuring clear United Nations systemwide roles and responsibilities; rapidly resetting preparedness and response strategies during health emergencies; and, enhancing United Nations system leadership for preparedness, including through routine simulation exercises. WHO should introduce an approach to mobilize the wider national, regional and international community at earlier stages of an outbreak, prior to a declaration of an IHR (2005) Public Health Emergency of International Concern.
Progress indicator(s) by September 2020
• The Secretary-General of the United Nations, with the Director-General of WHO and Under-Secretary-General for Humanitarian Affairs strengthens coordination and identifies clear roles and responsibilities and timely triggers for a coordinated United Nations systemwide response for health emergencies in different countries and different health and humanitarian emergency contexts. • The United Nations (including WHO) conducts at least two system-wide training and simulation exercises, including one for covering the deliberate release of a lethal respiratory pathogen. • WHO develops intermediate triggers to mobilize national, international and multilateral action early in outbreaks, to complement existing mechanisms for later and more advanced stages of an outbreak under the IHR (2005). • The Secretary General of the United Nations convenes a high-level dialogue with health, security and foreign affairs officials to determine how the world can address the threat of a lethal respiratory pathogen pandemic, as well as for managing preparedness for disease outbreaks in complex, insecure contexts.
The chances of a global pandemic are growing. While scientific and technological developments provide new tools that advance public health (including safely assessing medical countermeasures), they also allow for disease-causing microorganisms to be engineered or recreated in laboratories. A deliberate release would complicate outbreak response; in addition to the need to decide how to counter the pathogen, security measures would come into play limiting information-sharing and fomenting social divisions. Taken together, naturally occurring, accidental, or deliberate events caused by high-impact respiratory pathogens pose “global catastrophic biological risks.” (15)
The world is not prepared for a fast-moving, virulent respiratory pathogen pandemic. The 1918 global influenza pandemic sickened one third of the world population and killed as many as 50 million people – 2.8% of the total population (16,17). If a similar contagion occurred today with a population four times larger and travel times anywhere in the world less than 36 hours, 50 – 80 million people could perish (18,19). In addition to tragic levels of mortality, such a pandemic could cause panic, destabilize national security and seriously impact the global economy and trade.
Trust in institutions is eroding. Governments, scientists, the media, public health, health systems and health workers in many countries are facing a breakdown in public trust that is threatening their ability to function effectively. The situation is exacerbated by misinformation that can hinder disease control communicated quickly and widely via social media.
“Who could’ve seen it?!” – September 2019 version“Independent” 😉
No, they are not worried about misinformation. They are worried about their agenda being countered by truths leaking out on social media.
In the “Progress to Date” section, we find the following snippet (page 19):
In 2017 Germany, India, Japan, Norway, the Bill & Melinda Gates Foundation, the Wellcome Trust and the World Economic Forum founded the Coalition for Epidemic Preparedness Innovations (CEPI) to facilitate focused support for vaccine development to combat major health epidemic/pandemic threats.
On page 25, they are worried about armed resistance to their imposition of vaccines. To quote,
Challenges to poliomyelitis (polio) eradication efforts in Afghanistan and Pakistan and those experienced while containing the tenth Ebola outbreak in the DRC vividly demonstrate the impact that a breakdown in citizens’ trust and social cohesion can have on health emergency response. Consequences include attacks on both national and international health-care workers and delays or stoppages in response efforts. In some countries, waning trust in public health and government officials together with cultural and religious beliefs lead to is decreasing vaccination rates and leading to the re-emergence of measles and other vaccine-preventable diseases, a phenomenon found in communities at all economic and educational levels.
Page 34 proposes making ’emergency preparedness” a precondition for receiving loans and financial support from the IMF and the World Bank. To quote,
To mitigate the severe economic impacts of a national, regional epidemic and/or a global pandemic, the IMF and the World Bank must urgently renew their efforts to integrate preparedness into economic risk and institutional assessments, such as the IMF’s next cycle of Article IV consultations with countries, and the World Bank’s next Systematic Country Diagnostics for IDA credits and grants. The funding replenishments of the IDA, Global Fund to Fight AIDS, TB and Malaria, the and Gavi Alliance should include explicit commitments regarding preparedness.
Now here are the wonderful people who are members of the Global Preparedness Monitoring Board. Remember Fauci? Remember the Bill Gates Foundation? Other notables include a member of the Communist Party of China.
“Simulation exercises have been identified as a key voluntary instrument in the validation of core capacities under the “Implementation of the International Health Regulations: Draft 5-year draft global strategic plan to improve public health preparedness and response”, which was adopted by the seventy first World Health Assembly. Simulation exercises, along with After Action Reviews, represent the functional assessment of capacities and complement States Parties annual reporting, independent reviews, and joint external evaluations. They play a key role in identifying the strengths and gaps in the development and implementation of IHR capacities and to support countries to assess the operational capability of their national capacity for public health preparedness and response.” – WHO
Full-scale/field exercises (FSX): “A full-scale exercise simulates a real event as closely as possible and is designed to evaluate the operational capability of emergency management systems in a highly stressful environment, simulating actual response conditions. This includes the mobilization and movement of emergency personnel, equipment and resources. Ideally, the full-scale exercise should test and evaluate most functions of the emergency management plan or operational plan. Differing from the FX, a full-scale exercise typically involves multiple agencies and participants physically deployed in an exercise field location.” – WHO
WHO elaborates on what a SimEx is in October 2019
Field exercises: “See full-scale exercise. A field exercise is one form of full-scale exercise, focusing on more specific capacities or series of capacities, such as procedures for Rapid Response Teams (RRT), laboratory analysis or other sample collection and transport.”- WHO
Exercises are not one-time events, but should be undertaken as part of a carefully designed exercise program which ensures a common strategic objective is addressed. A comprehensive exercise program is made up of progressively complex exercises, which build upon the previous, until they are as close to reality as possible. This ‘building-block approach’ should start with basic exercises that test specific aspects of preparedness and response, followed by progressively complex exercises requiring additional preparation time and resources.
The figure below provides an illustration of the level of preparation and capacity needed for each exercise type.
Situation map as of September 10, 2020. US, Brasil, Australia, Scandinavia and other countries seem to conduct their own drills following a different agenda, and that matches the actual field situationSo what is WHO planning out for Ukraine?Ukraine is certainly being “groomed” for a 2nd wave of Covidiocracy. SourceWHO has been laying out the plans to control mass gatherings since 2019Read moreRead moreSource
“The exercise, code named “Crimson Contagion,” had eerie similarities to the current real-life coronavirus pandemic.
The exercise involved officials from more than a dozen federal agencies, several states and hospitals responding to a scenario in which a pandemic flu that began in China was spread by international tourists and was deemed a pandemic 47 days after the first outbreak. By then, in the scenario, 110 million Americans were expected to become ill.
The simulation that ran from January to August exposed problems that included funding shortfalls, muddled leadership roles, scarce resources, and a hodgepodge of responses from cities and states, according to the dunning assessment obtained by the Times.
It also became apparent that the U.S. was incapable of quickly manufacturing adequate equipment and medicines for such an emergency, according to the draft report.
White House officials told the Times that an executive order following the exercise improved the availability of flu vaccines. The administration also said it moved this year to increase funding for a pandemic program in HHS.
But Trump’s administration eliminated a pandemic unit within the Department of Homeland Security in 2018. And weeks after the first real coronavirus case was diagnosed in the U.S., Trump submitted a 2021 budget proposal calling for a $693.3 million reduction in funding for the Centers for Disease Control and Prevention.
Officials wouldn’t explain why the administration’s coronavirus response was so slow to roll out testing, or to move on promoting social distancing and school closings — all steps highlighted in the exercise, according to the Times.
While President Donald Trump has claimed that “nobody knew there would be a pandemic … of this proportion,” that’s exactly the kind of possibility the exercise addressed.
The Trump administration also had the benefit of lessons learned by the Obama administration in dealing with the Ebola crisis. Obama aides in early 2017 ran an exercise for pandemic preparedness for incoming officials of the Trump administration as part of the transition, but almost all of the previous administration’s experts had left the government by last year.
Former Director of National Intelligence Dan Coats, who was fired by Trump in 2019, warned of the danger of a pandemic to an unprepared nation last year in his Worldwide Threat Assessment.” – HUFFPOST
The photo above represents “The Department of Health and Human Services’ Covid-19 operations center in Washington. The department ran an extensive exercise last year simulating a pandemic” – NY Times
“The exercise played out in four separate stages, starting in January 2019.
The events were supposedly unspooling in real time — with the worst-case scenario underway as of Aug. 13, 2019 — when, according to the script, 12,100 cases had already been reported in the United States, with the largest number in Chicago, which had 1,400.
The fictional outbreak involved a pandemic flu, which the Department of Health and Human Services says was “very different than the novel coronavirus.” The staged outbreak had started when a group of 35 tourists visiting China were infected and then flew home to Australia, Kuwait, Malaysia, Thailand, Britain and Spain, as well as to the United States, with some developing respiratory symptoms and fevers en route.
A 52-year-old man from Chicago, who was on the tour, had “low energy and a dry cough” upon his return home. His 17-year-old son on that same day went out to a large public event in Chicago, and the chain of illnesses in the United States started.
Many of the moments during the tabletop exercise are now chillingly familiar.
In the fictional pandemic, as the virus spread quickly across the United States, the C.D.C. issued guidelines for social distancing, and many employees were told to work from home.” – NY Times
I’m not making any claims regarding how much did Trump play by that book, worth noting it existed and it got passed on
the ‘Event201’ exercise
We got banned for this! WEF openly admitted they ran a massive viral pandemic simulation in 2019
According to their own website, “Event 201 was a 3.5-hour pandemic tabletop exercise that simulated a series of dramatic, scenario-based facilitated discussions, confronting difficult, true-to-life dilemmas associated with response to a hypothetical, but scientifically plausible, pandemic. 15 global business, government, and public health leaders were players in the simulation exercise that highlighted unresolved real-world policy and economic issues that could be solved with sufficient political will, financial investment, and attention now and in the future.
The exercise consisted of pre-recorded news broadcasts, live “staff” briefings, and moderated discussions on specific topics. These issues were carefully designed in a compelling narrative that educated the participants and the audience.
The Johns Hopkins Center for Health Security, World Economic Forum, and Bill & Melinda Gates Foundation jointly propose these recommendations.”
Purpose
In recent years, the world has seen a growing number of epidemic events, amounting to approximately 200 events annually. These events are increasing, and they are disruptive to health, economies, and society. Managing these events already strains global capacity, even absent a pandemic threat. Experts agree that it is only a matter of time before one of these epidemics becomes global—a pandemic with potentially catastrophic consequences. A severe pandemic, which becomes “Event 201,” would require reliable cooperation among several industries, national governments, and key international institutions.
Similar to the Center’s 3 previous exercises—Clade X, Dark Winter, and Atlantic Storm—Event 201 aimed to educate senior leaders at the highest level of US and international governments and leaders in global industries.
It is also a tool to inform members of the policy and preparedness communities and the general public. This is distinct from many other forms of simulation exercises that test protocols or technical policies of a specific organization. Exercises similar to Event 201 are a particularly effective way to help policymakers gain a fuller understanding of the urgent challenges they could face in a dynamic, real-world crisis.
“The next severe pandemic will not only cause great illness and loss of life but could also trigger major cascading economic and societal consequences that could contribute greatly to global impact and suffering. The Event 201 pandemic exercise, conducted on October 18, 2019, vividly demonstrated a number of these important gaps in pandemic preparedness as well as some of the elements of the solutions between the public and private sectors that will be needed to fill them. The Johns Hopkins Center for Health Security, World Economic Forum, and Bill & Melinda Gates Foundation jointly propose these recommendations.”
Audience
An invitation-only audience of nearly 130 people attended the exercises, and a livestream of the event was available to everyone. Video coverage is available here.
Exercise team
Eric Toner, MD, is the exercise team lead from the Johns Hopkins Center for Health Security. Crystal Watson, DrPH, MPH and Tara Kirk Sell, PhD, MA are co-leads from the Johns Hopkins Center for Health Security. Ryan Morhard, JD, is the exercise lead from the World Economic Forum, and Jeffrey French is the exercise lead for the Bill and Melinda Gates Foundation.”
Main organisers: The Johns Hopkins Center for Health Security, World Economic Forum, and Bill & Melinda Gates. World Economic Forum as in the ideologists that redacted The Great Reset.
In order to create momentum for the Great Reset, UK royal Prince Charles said the imagination and will of humanity “will need to be captured” so that they can set the world on a new trajectory. This is taken from his historical but largely ignored speech at the official launch event for The Great Reset.
He further suggested that longstanding incentive structures that have adverse effects on the environments must be reorientated, and that systems and pathways will need to be redesigned to advance net zero emissions globally.
“This reset moment is an opportunity to accelerate and align our efforts to create truly global momentum. Countries, industries and businesses moving together can create efficiencies and economies of scale that will allow us to leapfrog our collective progress and accelerate our transition,” the Prince said.
NEW – At COP26, The most powerful private financial interests in the world announced a plan to transform the global financial system by fusing w institutions like the World Bank and using them to further erode national sovereignty in the developing world.https://t.co/8rqDME4OVj
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Make a blog post on WordPress or anywhere you can get good live traffic reports. Set it private so that no one can find the link unless you give it to them.
Make a Facebook post with that link and boost it. Make sure there’s no other links included so the audience can’t go anywhere else
Compare the Facebook link click reports with the other traffic reports you have available for your website.
On the last test we did, Facebook reported 326 link clicks, WordPress 20, for the same timeline. This costed us almost $30 from your donations but I think it’s the best spent money on Facebook from all we ever did.
These are the people who “fact-check” us. Any number or claim ever presented by Facebook is worthless. Facebook is nothing but a Narrative Enforcement & Smear machine literally stealing money, health and life from people by faking everything it touches.
Ever felt fringe, overwhelmed by drones, marginalised? You’re just being gas-lighted by Facebook, Google and an army of trolls whose very own existence proves our reality is fabricated and rigged.
In the figure above we have Dork Suckerborg, Lord of the Echo-chambers, trying to tell us we made 7,000+ views without a single reaction or comment. As if that’s even possible. If I showed 7,000 people a blank page, at least 100 would react (mostly angrily I guess).
The “virality circuit breaker”, from our close observations, comes out to be a little program meant to lie about your interactions, as a tool to stop people from following up and engaging with each other, increasing the popularity of some posts.
Imagine getting 115k likes and no heart 😀 What numbers do you see? Check it here
The problem is the mental ret@rdation the elites promoted in the masses trickled up into their own business and now they are way too stupid to accomplish anything that’s not based on brute force. So what happens is that, especially when there’s many interconnections on a post, the lie you tell one user needs to be propagated to all the network. But the same lie doesn’t work the same for everyone. You need to customise the lie to make it plausible for everyone. And if they weren’t dead inside, they could’ve tell from the guts their AI and any machine will fail at this task, because so much human variability is uncomputable. This is how, eventually, our humanity will beat the borg. This is why they want to eliminate the differences between us and turn the collective mental into an uniform marmalade: less variability to compute and manage, less resources and costs invested, less worries. But because of the generalised mental underdevelopment, there will be billions of victims in the process of winning. And everyone basing anything on Facebook or Google numbers will be a victim of some sort too.
Let’s see another instance of gaslighting attempted on us: In the image above witness Facebook trying to BS us that no one gives a crap about our post. A few thousand people interacted with it, in fact. Some were my or my friends’ profiles. None of the numbers we seen on the reports matched the same reports sent to others, or even to ourselves, like the notification on the profile didn’t match the one on the page nor the one on the feed. The lie is too big and intricate to manage with their fake ass quantum computing The machine failed countless times at covering its tracks. We recorded tons of these failures. They figured it out some days ago but now then patches made it worse, so at times they break the notifications completely, it’s still better than you seeing the king naked.
NEK – Narrative Enforcement Korps (I just made this name up but they’re real)
Get involved, share this as wide as you can, let’s crash this monster and its stock market value by outing its schemes!
Our worldwide readership is told to its face they are not going to show our link in comments
Sometimes it feels like Fakebook is holding meetings in which they debate how to help us further expose them. The main problem remains the public’s functional illiteracy which disables their cognitive abilities when facing evidences of wrongdoing
This called for a new Facebook cover, feel free to download and use 😉
In a coming episode we hope to teach you similar tricks for Google, who hides it better, but it’s just as rigged. Way more complicated to prove.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
These links from their website are all I have for now, but it’s sufficient evidence. I found it important to let it all out ASAP, while I dig for more relevant info.
I find very interesting who the main traders are: Switzerland ($23,684,716.51K , 2,538,500 Kg), Germany ($17,464,406.19K , 7,242,210 Kg), European Union ($16,940,789.16K , 8,953,990 Kg), United States ($8,283,146.64K , 7,020,260 Kg), Ireland ($6,356,054.92K , 590,259 Kg).
China has been shipping Rona tests like there’s no tomorrow since 2018:
UPDATE SEPT 9, 2020 I think you will find this WB document very interesting. Download PDF
“This document describes a programmatic framework responding to the global coronavirus (COVID-19) pandemic, the ‘COVID-19 Strategic Preparedness and Response Program (SPRP)’, which utilizes the Multiphase Programmatic Approach (MPA), to be supported under the FTCF. The proposed Program, by visibly committing substantial resources (IBRD/IDA financing for SPRP is US$6 billion), and complementing funding by countries and activities supported by other partners, would help ensure adequate resources to fund a rapid emergency response to COVID-19. In parallel, it is being submitted for approval the financing of Phase 1 of the Program for 25 Investment Project Financing operations under the SPRP for countries across the world. The 25 countries are: Afghanistan, Argentina, Cabo Verde, Cambodia, Congo Democratic Republic of, Djibouti, Ecuador, Ethiopia, Gambia, Ghana, Haiti, India, Kenya, Kyrgyz Republic, Maldives, Mauritania, Mongolia, Pakistan, Paraguay, San Tome & Principe, Senegal, Sierra Leone, Sri Lanka, Tajikistan, and Yemen (the list of country operations is in Annex I of this document and the country operations are described in their respective Project Appraisal Documents (PADs)). The PADs for the 25 country projects included in this Phase 1 package are available online.”
The Covid Circus is supposed to be about health, but it’s ran by financiers and royalties, fronted by a computer dork and a communist terrorist.
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
Don’t want your posts reported or your profile flagged because you’re critical of Pharmafia, the establishment and their fake news? Block these profiles. Permanently updated, there’s thousands of them. The secret agents of the narrative enforcement, the real Covidiocracy army.
Funnier than the meme is the fact that this used to be a profile pic for a troll
More to come, just started to get things organised
To be continued? Our work and existence, as media and people, is funded solely by our most generous supporters. But we’re not really covering our costs so far, and we’re in dire needs to upgrade our equipment, especially for video production. Help SILVIEW.media survive and grow, please donate here, anything helps. Thank you!
! Articles can always be subject of later editing as a way of perfecting them
















![[Exclusive] Trump officially endorsed by the new Master of the Knights Templar](https://silview.home.blog/wp-content/uploads/2020/10/templar-cover-2.jpg?w=1024)
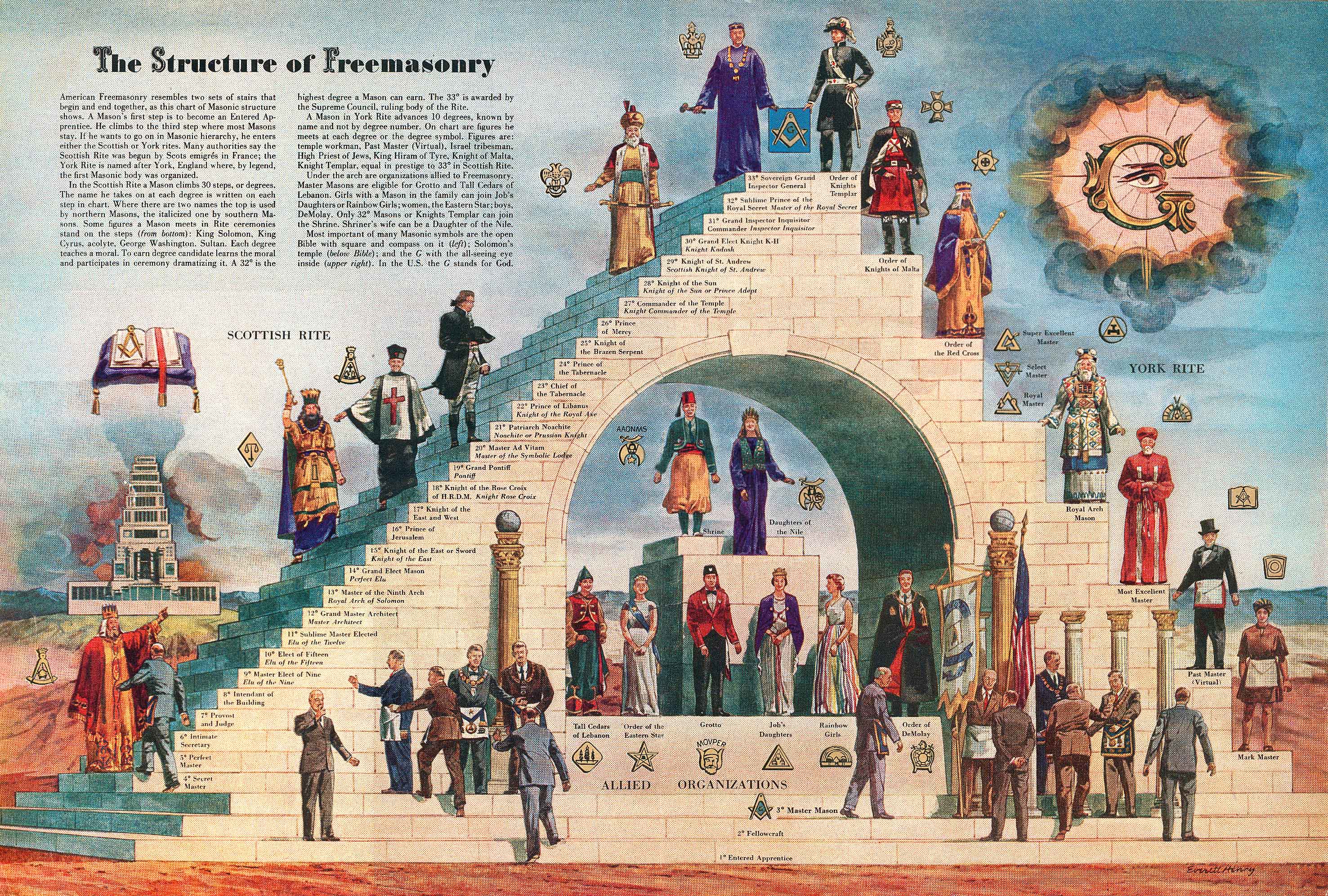


















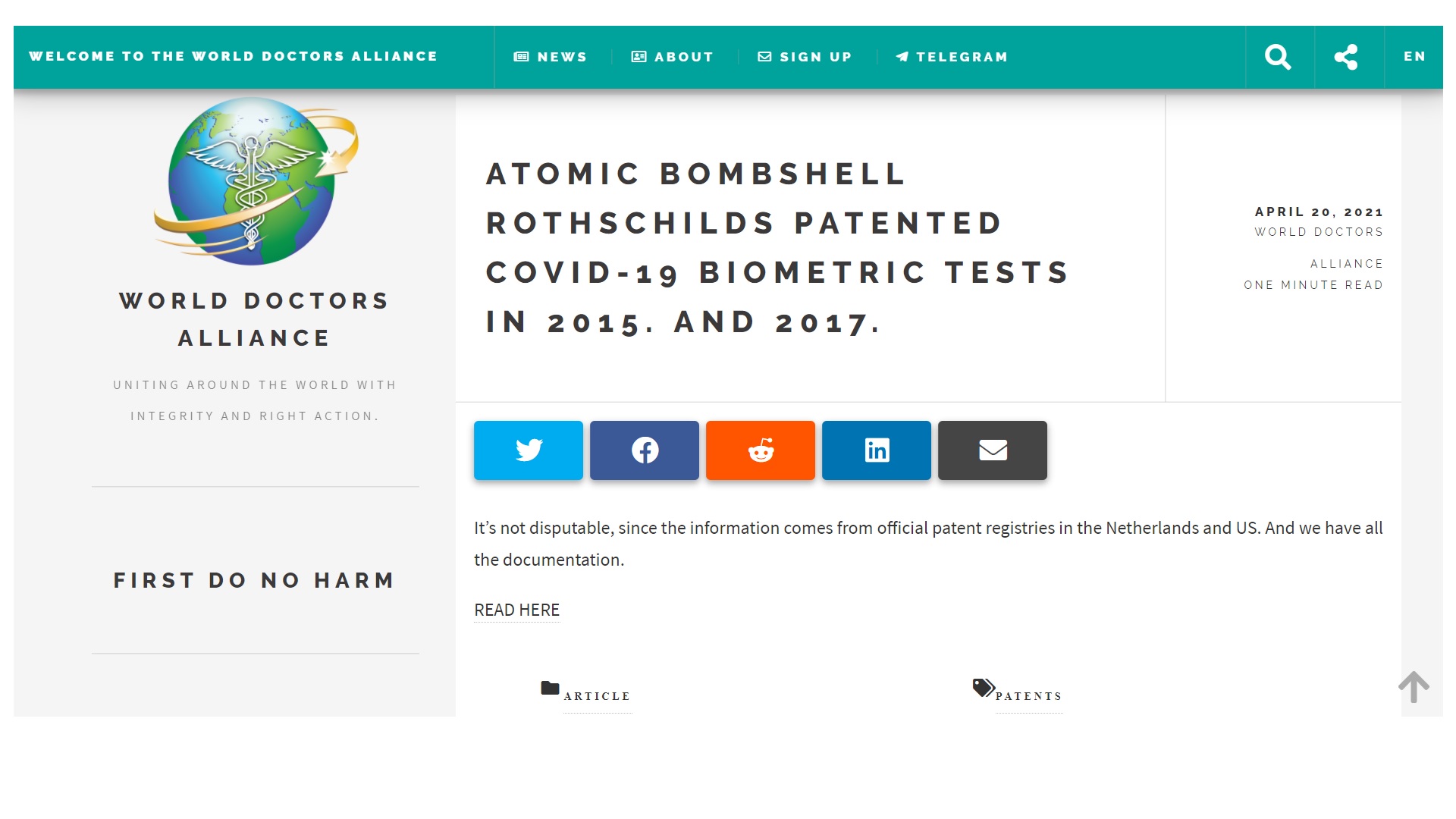









































![[Exclusive] Final Evidence Covid-19 Is A ‘SimEx’ – Planned Simulation Exercise by WHO and World Bank](https://silview.home.blog/wp-content/uploads/2021/01/wb-stanford-shift.jpg?w=1024)








































![[Updated] World Bank says Covid-19 test kits are being sold since 2017](https://silview.home.blog/wp-content/uploads/2020/09/wb-covid-1.jpg?w=1024)









{kind=link}
{kind=link}